I spent a week and a half hospitalized for depression as an inpatient at a behavioral health hospital, and all I got was a lot of decaf, terrible antiperspirant, and ungroomed eyebrows (dangerously close to being “eyebrow”). Oh, and a will to live.
When I ran out of methylfolate, my mutant brain began to rebel. All of the work I had done to pull myself out of the dark pit of depression flew out the window as my symptoms came roaring back. I was tired of living with the darkness, the fatigue, the brain fog, and the sadness of depression. And, because it seemed that there was no other way to live, I was tired of living. I fell into the old habits of isolating, harming myself, and outwardly presenting as if everything were fine.
When you stuff everything down, at some point you run out of space. My tipping point came during my weekly therapy session. After describing the hopelessness and elaborating on the details of my thoughts about suicide, my therapist convinced me to go to the hospital. Once I had been assessed, I was given the choice (that wasn’t really a choice) to either sign myself in voluntarily or be put on a 72-hour hold. I signed myself in.
The unit I was on is designed to be a crisis stabilization unit. There’s no one-on-one therapy, visiting hours are actually a singular visiting hour each day, and the items you’re allowed to have are extremely limited. Patients are expected to be in group therapy, meeting with a doctor or social worker, or working on an alternate activity like journaling. You are locked out of your bedroom for most of the day, so your options for privacy are slim to none. You and your roommate must sleep with the door open, as nurses walk around all night long doing “checks,” where they mark down your whereabouts and what you’re doing on their clipboard paperwork. Not to mention your bed is hard and noisy, and your pillow feels like a sack of uncooked rice. It was a difficult environment to be in for 11 days, to say the least.
Being hospitalized for depression is not easy, but the good news is, it works. I switched medications, and while it’s too soon to say whether it’s a good fit for me, being kept in a safe place surrounded by people who understood what I was going through went a long way towards getting me back on my feet. The groups tended to cover topics that were familiar to me, so not much of the information was new. That being said, hearing other patients’ perspectives and experiences was what made my stay helpful.
I stayed for several days longer than the average at that hospital. The staff wanted to see more improvement than I was making, and I wanted to avoid triggering a 72-hour hold by declaring that I was checking out against medical advice. This resulted in my estimated discharge date being pushed out a day or two at a time while my frustration levels grew. Eventually, I agreed to do a partial hospitalization program at a different facility near where I live. This was enough to convince the staff that I was safe to go home. Today, I start the process of doing a PHP. I feel much better than I did when I was admitted to the hospital. I know that shifting back into my normal routines will be a tricky transition and that a week and a half in a hospital doesn’t fix everything. But, it’s a start.
We all have those sneaky thoughts that come unbidden when we make a mistake or are faced with a change. I don’t know a single person who hasn’t mentally beat themselves up over a perceived shortcoming. Often, it isn’t deserved. But when your automatic thoughts are that you deserve those thoughts, what do you do?
“Automaticity is granted if the perceiver lacks awareness of the process, does it with efficiency (i.e., with minimal use of cognitive resources), has no intention to do it, or cannot control it.”
Based on this definition, automatic thoughts include those about others, such as deeply held prejudices. It also includes the intrusive thoughts that characterize Obsessive Compulsive Disorder, but I’ll be focusing more on those automatic thoughts that don’t necessarily play a direct role in psychopathology. For example, self-referential thoughts like, “I’m going to fail this exam. I always fail.” Those are the types of thoughts I’m talking about here.
Negative Automatic Thoughts
The most well-known measure in this area is the Automatic Thoughts Questionnaire (ATQ), a 30-item instrument developed in 1980. The ATQ contains statements like “I am a failure,” and asks participants to rate each statement on a scale representing the frequency with which they experience that thought. It’s a cross-validated questionnaire that’s been shown in several studies to correlate with depression and separate depressed from non-depressed individuals.
When presented with a distressing stimulus, previously depressed participants and people who have never been depressed experienced stronger belief in negative automatic thoughts. The researchers propose that cognitive reactivity is related to relapse and recurrence of depression.
Cognitive reactivity refers to the triggering of negative thought patterns by small declines in mood. The ability to resist slipping into negative cognitions seems to have a protective effect; inpatient surveys taken at two time points show that decreases in negative automatic thoughts are strongly correlated with reduced suicidal ideation.
Positive Automatic Thoughts
The relationship between negative automatic thoughts and depression and anxiety is well documented. We can infer that the lackof negative automatic thoughts has beneficial effects on mental health, but this still isn’t quite the same as the presence of positive automatic thoughts. However, research does support the assumption that positive thinking is related to positive mood. A variation of the ATQ was developed to measure positive automatic thoughts. It’s called the ATQ-P, and higher scores on it are strongly associated with lower levels of depression. A healthy balance of positive and negative thoughts appears to be weighted toward more positive than negative- a ratio of 0.62 to 0.38, to be exact (according to one study).
Where Exactly Do Automatic Thoughts Come From?
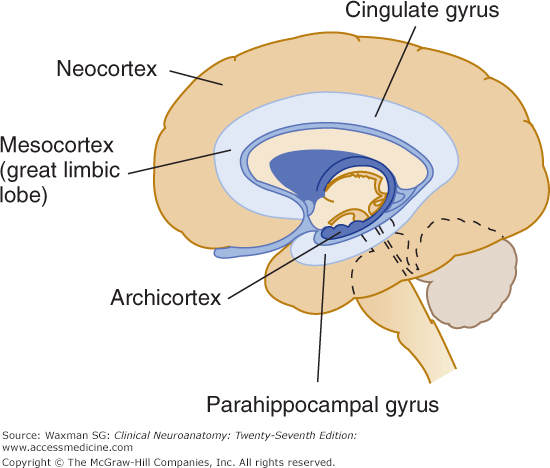
Parahippocampal gyrus
One area of the brain that is linked to automatic thoughts is the parahippocampal gyrus, a part of the limbic system.
“The voxel-based morphometry results showed that the GMV of the right parahippocampal gyrus and fusiform gyrus and the WMV of the right superior temporal pole increased with the severity of depression.”
Let’s break that down. A voxel is a value assigned to a three-dimensional grid. Think “pixel” but with volume. Voxel-based morphometry is a technique for assessing differences in brain volume. Brain scans are registered to a standard, voxel-based template, then each voxel is “smoothed” by averaging it with the values of the surrounding voxels. Finally, the image volume of each scan is compared to the other scans’ volumes and the differences between voxels are evaluated statistically. Basically, it’s a way to quickly compare lots of structural brain scans using computers.
The study found that increases in the volume of grey and white matter in certain regions of the limbic system are associated with increasing severity of depression, as measured with the ATQ. So, negative automatic thoughts are associated with depression, and depression is associated with higher volume in the emotional center of the brain. That doesn’t necessarily mean that negative automatic thoughts are directly related to grey and white matter volume. Or does it?
Statistical tests showed that the combination of automatic thoughts and grey matter volume in the parahippocampal gyrus predicted depression measured by the ATQ and the Self-Rating Depression Scale. The automatic thoughts mediate the relationship between volume and depression. They also seem to mediate the relationship between neuroticism and depression.
Medial Prefrontal Cortex
The medial prefrontal cortex is not part of the limbic system. It’s located at the very front of your brain and is associated with the processing of social information. Hyperactivity in this region has been linked to neuroticism and self-generated thought. The tendency to worry and impose self-generated beliefs onto a reality that doesn’t match those beliefs sounds a lot like the automatic thoughts in the studies above. But it’s not all bad; the same hyperactivity and self-generated thoughts are also associated with creativity.
Combatting Negative Automatic Thoughts
Hopefully, you haven’t read all of that and decided that the next time someone tells you to be more positive you’ll just say “the grey matter in my parahippocampal gyrus says, ‘No can do.'”
Photo by @linkedinsalesnavigator on Unsplash
Cognitive behavioral therapy has been shown to result in reductions of automatic thoughts and dysfunctional attitudes associated with non-clinical depression. CBT makes use of behavioral experiments and automatic thought records. People perceive behavioral experiments to be more powerful than combatting automatic thoughts with logic alone, which could be because behavioral experiments function through emotion-based cognitive systems. Mindfulness has also been shown to reduce automatic thoughts, and it’s associated with increased life satisfaction.
There are plenty of reasons to believe that we have the power to effect change in our own brains.
What helps you recognize negative automatic thoughts, and how do you practice self-compassion?
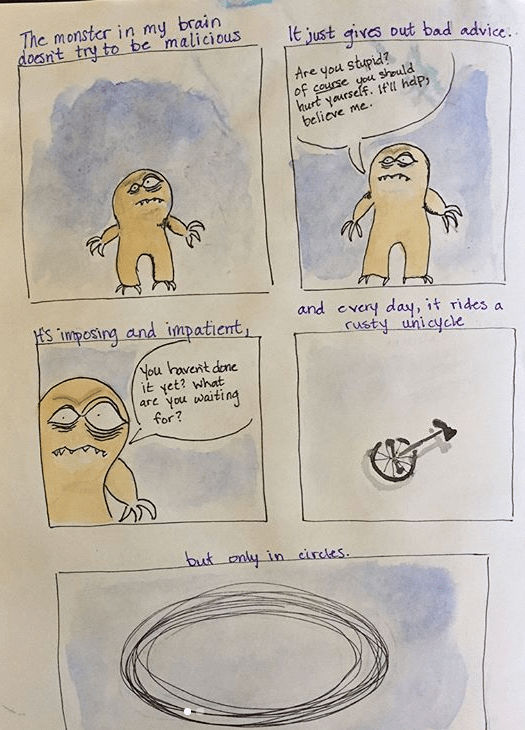
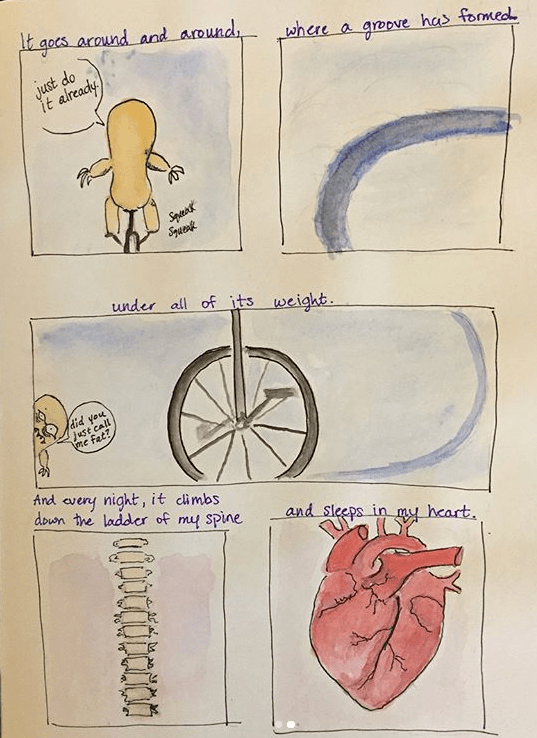
What is a lumpdate? I’m glad you asked. “The Lump” is the name I use to refer to the imaginary goblin in my brain that rides a tiny, rusty unicycle in circles, day and night.
The Lump was quiet for a while, but it’s back again, so this is a lumpdate- an update about the Lump. It won’t be a long lumpdate; the Lump is rather unoriginal and doesn’t have many new points to make. Really, they’re all repeats of the same damaging doubts from before.
In sum, the Lump is back, setting up shop in my mind.
I’d like to introduce you to my irrational brain, partly to illustrate how distorted depression can make your thoughts, and partly to convince myself that this will pass. I take methylfolate because I’m a mutant and it helps my antidepressants work better. I ran out a couple of weeks ago and was slow to get it refilled. There aren’t any withdrawal symptoms of going cold-turkey because it’s really more of a supplement than anything else. (I’m much more careful about my other medications; you should never stop taking antidepressants suddenly without the supervision of your doctor.)
In any case, I didn’t call right away to get my methylfolate refilled. Initially, I thought that it would surely stay in my system for a few days and that it wouldn’t be a big deal to go without it briefly. In hindsight, that was a mistake. It was ok for a few days, but once I started to feel my depression worsen, I started to think some really unhelpful thoughts.
I messed up by not being on top of my responsibilities health-wise. This is my fault. I deserve to feel this. Therefore, I should not refill this medication, so as to prolong my suffering and punish myself.
Uh, no. Just… no. This is rational brain speaking. The statements above are utter nonsense and are not helpful in the slightest.
While I know that the most logical explanation for this decline in my mood is the lack of that medication, irrational brain whispers that maybe it’s just me. And that just in case it’s not me, and the arrival of that medication marks an end to this little blip, now’s my chance to self-destruct.
Seriously. Where do these thoughts come from?! Here’s another example: I was sitting outside with my dog and realized I hadn’t had any water in a while. Out of nowhere, my irrational, depressed brain said I deserve to be thirsty.
Apparently, I should just completely deprive myself of all comfort and nourishment, because according to my automatic thoughts, I’m a terrible person.
My meds have arrived, so the thing to do now is to try not to listen to myself until they kick in. Much easier said than done. In the meantime, I’m doing my best. That’s all we can ever do.
I’m hoping to make this the first post in a series called “Science Saturdays” (now taking suggestions for a more creative name) where I dive into the research at the intersection of mental health and (fill in the blank). I dipped my toes into these waters with previous posts like “Pets and Mental Health“, “Can You ‘Grow Out Of’ Childhood OCD?“, and “What’s the Deal with MTHFR and Psychiatric Conditions?” My intention is to take an objective look at recent research, let it percolate through my noggin while I sift through the dozens of tabs I’ve amassed in Google Scholar, then report back with what I think are some important takeaways.
Here in the northern hemisphere, we’re perched on the cusp of spring, and boy, am I ready to get outside. I live in Colorado, and hiking is one of, if not the most, enjoyable ways I spend my time in the warmer months. I’ve been gazing longingly at the mountains, perusing dog backpacks (that’s backpacks for dogs to wear) on Amazon, and figuratively dusting off my trail map app in anticipation. It could just be that I’m particularly drawn to being outside because of my personality and upbringing, but I’ve recently come across some buzz surrounding the positive effects that nature has on our emotional and physical health. So, I figured, what better way to become even more entrenched in spring fever than to spend a few hours reading about the outdoors?
Nature and Physical Health Studies
Nearly every article I’ve read so far has referenced a study published in 1984 by RS Ulrich. The study looked at a group of 46 hospital patients, all of whom had their gallbladders removed and were monitored postoperatively. 23 patients stayed in rooms with views of trees, while the other 23 had views of a brick wall. The now classic study found that the patients who had views of trees recovered faster and required less pain medication than the other group of patients.
Increasingly, researchers are investigating the relationship between biodiversity in green spaces and psychological benefits. Several nature and mental health studies have found significant associations between higher plant and bird diversity and positive mental effects. A 2007 study by Fuller et al. found a positive correlation between plant species richness and participants’ sense of identity and ability to reflect. The 312 participants were fairly accurate at assessing plant species richness, which muddies causality. The question then becomes: are the benefits derived from species richness or perceived species richness?
Here’s another study to elaborate on that distinction. Researchers here found that psychological benefits of nature exposure were correlated not with biodiversity, but with participants’ perception of biodiversity only. In this study, participants were apparently not at all good at estimating species richness, and it affected their experience of being outside, regardless of how many species were actually present.
Frequency and Duration of Nature Exposure
So it seems that the more varied and species-rich the environment, the better. But is glancing out a window now and then the same as going for a walk outside, psychologically? I’d say no, but that doesn’t mean that short exposures to nature don’t benefit us. After all, just a 40-second break to look at a green, plant-filled roof has been shown to improve attention and performance on cognitive tasks, as compared to a break of the same length with views of concrete roofs.
In a sample of over 1500 Australian respondents, longer duration of nature excursions is associated with decreased prevalence of depression and high blood pressure. More frequent visits to public green spaces are associated with a greater sense of social cohesion, which I imagine contributes positively to mental health in general.
Criticisms of Nature and Mental Health Research
Few studies on the topic of nature and mental health take an epidemiological approach, leading some to point out that we have very little data on long-term, population-level health effects of nature exposure. Criticisms of some studies also include sample size, lack of adequate controls, and statistical rigor. However, the number of studies that demonstrate a correlation between nature and mental health benefit vastly outweigh the number of studies that show no relationship. While this does not negate the weaknesses mentioned previously, it does seem to suggest that there is validity to the idea that nature is emotionally beneficial.
The Daffodils are Blooming
All the signs that winter is ending are here; the daffodils are blooming, more birds are singing, the neighbors are cleaning out their garage, and before spring really gets underway, Colorado is scheduled to get one or two more last-minute dumps of snow.
Speaking of, now that I’ve gotten myself extra excited to get outside and let my brain soak in the wonderful sights, sounds, and smells of spring, it’s time to prepare myself for tonight’s snowstorm.



 The remnants
The remnants