It’s nothing to be ashamed of I tell myself twice daily. What day is it? They all blend together. I open the third compartment, pour the pills into my palm, wait for a moment. Maybe this day will be the day. Maybe if I give the medicine a moment of silence; infuse it with my desperation before I let it fall down the dark well of my esophagus.
How many have I tried? Not enough that all hope is lost. How many have I tried? Enough that they call it “treatment resistant” depression. I call it drowning by degrees. Later, I open the third compartment, pour the pills into my palm, and wait a moment.
I’ve been enjoying all of the content online for Mental Health Awareness Month, and I thought I’d contribute my own story. Here’s my own experience of why advocating for yourself is important.
I have severe psoriasis, an autoimmune skin condition that makes itchy, flaky plaques where my skin cells regenerate too quickly. During my recent hospitalization (for severe depression), I let my doctors know about this in a brief, it’s-not-that-relevant-but-you-asked kind of way. When the psychiatrist asked if I had any physical conditions, I informed him of my psoriasis.
A few days later, I was meeting with my social worker to discuss my treatment plan. Under “diagnoses,” Major Depressive Disorder and psychosis were listed. Before I even said anything, my social worker quickly brushed it off and said, “Don’t worry too much about the psychosis- it might just be that you were confused when you came in.”
Now, I’m the kind of person who will eat the wrong food at a restaurant rather than speak up and point out a mistake. I’m the kind of person who willingly takes the middle seat on an airplane because my neighbor explains that she has to pee a lot. Seriously. I am not assertive.
However, diagnoses are a whole ‘nother bucket of fish. When I saw that on my treatment plan and heard my social worker minimize it, I made it clear that I was confused by it and wrote my concern in the questions portion of the form. The next time I saw the psychiatrist, I steeled myself in preparation to ask about the mysterious psychosis that I definitely didn’t have. Before I could bring it up, he sat down, sighed, and said, “It turns out that they couldn’t read my handwriting and thought I wrote ‘psychosis’ when really, I wrote ‘psoriasis.’ It’s all fixed, now.”
I laughed about it at visiting hour that night and for many nights after. Really, we’re still laughing about it. We’re getting some serious mileage out of that one.
The important thing is that I spoke up for myself and that it got remedied. I almost had an incorrect diagnosis which could have caused more confusion down the line. So, speak up! If something doesn’t look right or feel right, let your doctor know. They’re people too, and sometimes mistakes happen.
Also, handwriting is more important than you might think.
In light of my recent posts, I thought it might be useful to elaborate on the levels of mental health care you can find in a hospital setting (at least in the US). What are the differences between them, and what can you expect from each?
Inpatient Treatment
Entering a hospital as an inpatient for mental health care can be incredibly nerve-wracking. If you don’t know what to expect, the experience is overwhelming. The important thing to remember is that the system is designed to keep you and the other patients safe.
In an inpatient setting, you sleep at the hospital and spend your days on the unit. You might have a roommate; they’re probably just as overwhelmed as you are. The staff will likely elaborate on the expectations for patients, but you may be expected to spend the majority of your time in a common area, interacting with other patients and staff. Your nurses and doctors will want to see that you’re participating in group therapy, willingly spending time outside of your room, and eating meals with the unit. You’ll meet with your doctor and a social worker, and have a chance to discuss your treatment goals and any concerns you have. Different hospitals have different timeframes for this; you could meet with your doctor as often as every day, although it may happen less frequently.
Before you’re discharged, the staff will probably want to be sure that you have a support system, safety plan, and aftercare set up. Continuing mental health care might look like a partial hospitalization program, intensive outpatient program, or outpatient therapy with your own mental health counselor.
Partial Hospitalization Program (PHP)
The next level down from inpatient care is a partial hospitalization program. In a PHP, patients typically attend therapy for most of the day, sleep at home, then return for the next day of programming. For example, the PHP I did was from 9 am to 3 pm, Monday through Friday for ten days.
Programming usually focuses on teaching skills and information you can use to manage your illness. The PHP I was in took content mainly from DBT, although we also touched on ACT and CBT. You’ll meet with a psychiatrist and your case manager, who is usually one of the therapists who leads group discussions and teaches content. Your case manager will probably set up a treatment plan with you, and meet with you periodically to check in on your progress.
Many people come to a PHP through inpatient hospitalization. After spending time isolated from your normal, day-to-day life, it can be overwhelming to be tossed back into it. A PHP can serve as a helpful step-down to ease you back into your routine. Other people come straight from their outpatient treatment. They may not need the level of mental health care you get with inpatient treatment, but the support of a PHP can give them the structure they need to stay safe.
Intensive Outpatient Program (IOP)
In the same way that a PHP offers a transition from inpatient back into your normal life, an IOP does the same. It’s the next level down from a PHP, but is still, well, intensive. An IOP is similar to a PHP in the content that’s taught, but you meet less frequently and for a shorter amount of time each session, but for a longer overall duration. Many IOPs meet three times per week for three hours. The program might run for as many as eight weeks. The IOP at the hospital where I did my partial hospitalization had a more independent treatment; you didn’t get to meet with a psychiatrist or a case manager. That meant you would need to have outside medication management set up for your time in the IOP.
Many people go straight from inpatient treatment to an IOP, although others may need the structure of a PHP. Some people continue on from partial hospitalization to intensive outpatient, but sometimes that’s not feasible with work or family obligations. I decided not to do an IOP, but rather to return to my regular schedule and leave IOP as an option should I need more intensive mental health care down the road. It’s all very individual, and which program you choose depends on your specific needs and constraints.
Two or three days into my partial hospitalization program, it became clear to me that my peers were seeing positive results. At check-in, those closest to leaving would report feeling “good”, or “light”- two sensations that are unfamiliar to my depressed brain. I was glad that they were feeling better, and initially, it gave me a glimmer of hope for myself.
As the days passed, that hope dimmed; I wasn’t feeling much better at all. In fact, as my last day approached, I started feeling lower and lower. My thoughts about self-harm came back in full force, and when I tried to use the skills we’d been taught to combat them, I was unsuccessful. Morning check-in was even more excruciating than usual because I had to admit that I wasn’t doing well. The people who had come before me had felt better, so what was I doing wrong?
For one thing, I wasn’t doing anything “wrong”. The psychiatrist and both therapists for the program all agreed that the root cause of my depression is chemical. This doesn’t mean that coping skills are useless. They can help keep me safe and offer healthier alternatives to my go-to, maladaptive coping mechanisms. Over time, I can retrain my brain to help me get out of negative thought patterns or habits. However, coping skills are unlikely to do much to address the causative problem.
Secondly, there is no right pace for recovery. Comparing myself to others was only making me feel worse. That said, it’s only natural that we look to others to find out what to expect when we’re in an unfamiliar situation. I wish I had been able to temper my expectations when comparing myself to others in partial hospitalization.
Just because I didn’t leave partial walking on air doesn’t mean I “failed”. I still got a lot out of the experience.
Connection
Similar to my experience of being an inpatient at a mental hospital, one of the most valuable takeaways for me was the sense of connection I had with other patients. Hearing about other people’s perspectives on a shared experience helped me gain insight into my own thoughts and behaviors. Plus, it feels good to talk to people who understand your suffering and can empathize. I definitely came away from the ten-day program feeling less alone.
A sense of my own value
The first few days of my participation in the PHP, I was there for my family. I was there because other people wanted me to be, and I was willing to commit my time to a program like that in order to ease my family’s fears. A few days ago, though, I realized that I felt more like I was there for myself. It was a subtle shift, but it feels like a big step.
Acceptance
Throughout my inpatient hospitalization and partial hospitalization, I had several moments that stopped me in my tracks. The fact that I was at that level of care for my mental illness seemed surreal, and I couldn’t wrap my mind around the situation. I think that I have a better grasp on my symptoms and what I need to do to keep them under control. I also have a sense of acceptance that once I feel better, I’ll still need to manage my illness; I won’t be able to push returning symptoms under the rug. That’s how I ended up in the hospital.
Greater understanding of my patterns and behaviors
While the skills I learned may not address the root of my depression, they certainly help me shift my behavior towards healthy responses and actions. Perhaps the biggest behavioral takeaway for me is greater awareness of how I withdraw, isolate, and avoid addressing the issue of my depression with my loved ones.
Patience
No, I didn’t leave partial hospitalization feeling like my peers who had left before me. Everyone goes at their own pace, and everyone has unique circumstances and factors involved in their symptoms. All we can do is go day by day.
I’d like to introduce you to my irrational brain, partly to illustrate how distorted depression can make your thoughts, and partly to convince myself that this will pass. I take methylfolate because I’m a mutant and it helps my antidepressants work better. I ran out a couple of weeks ago and was slow to get it refilled. There aren’t any withdrawal symptoms of going cold-turkey because it’s really more of a supplement than anything else. (I’m much more careful about my other medications; you should never stop taking antidepressants suddenly without the supervision of your doctor.)
In any case, I didn’t call right away to get my methylfolate refilled. Initially, I thought that it would surely stay in my system for a few days and that it wouldn’t be a big deal to go without it briefly. In hindsight, that was a mistake. It was ok for a few days, but once I started to feel my depression worsen, I started to think some really unhelpful thoughts.
I messed up by not being on top of my responsibilities health-wise. This is my fault. I deserve to feel this. Therefore, I should not refill this medication, so as to prolong my suffering and punish myself.
Uh, no. Just… no. This is rational brain speaking. The statements above are utter nonsense and are not helpful in the slightest.
While I know that the most logical explanation for this decline in my mood is the lack of that medication, irrational brain whispers that maybe it’s just me. And that just in case it’s not me, and the arrival of that medication marks an end to this little blip, now’s my chance to self-destruct.
Seriously. Where do these thoughts come from?! Here’s another example: I was sitting outside with my dog and realized I hadn’t had any water in a while. Out of nowhere, my irrational, depressed brain said I deserve to be thirsty.
Apparently, I should just completely deprive myself of all comfort and nourishment, because according to my automatic thoughts, I’m a terrible person.
My meds have arrived, so the thing to do now is to try not to listen to myself until they kick in. Much easier said than done. In the meantime, I’m doing my best. That’s all we can ever do.
When I was 10, I felt compelled to tell my parents “I love you” every time they left the house. Going to the grocery store? I love you. Going to work? I love you. Going to the mailbox? I love you. The fear that something catastrophic will happen to family members is a common manifestation of childhood and adolescent OCD. I thought that if I failed to carry out this ritual, my parents wouldn’t know that I loved them if or when something terrible occurred.
I was also preoccupied with germs; my hands were cracked and bleeding from excessive washing, and I worried constantly about contamination. I always walked a specific pattern on the rug in the hallway, and I carefully watched the family dog to be sure I’d notice when he winked at me–so that I could wink back. I couldn’t tell you why I had to wink at the dog, I just had to.
I knew that these behaviors were irrational, and yet the anxiety it caused me to resist the compulsions seemed unbearable. I was afraid to go to sleep because I worried I might sleepwalk and harm my family in the middle of the night. Nearly every evening, I would tearfully confess my intrusive thoughts to my mother, convinced that she would be afraid of me for thinking such awful things. OCD commanded almost every aspect of my life.
Did I Grow Out Of It?
My parents tried to get me into therapy, but I was shy and ashamed, and simply refused to participate. So, I started taking an SSRI, slowly titrating up to the maximum dose. And incredibly, it worked. Suddenly, I was free from the torturous anxiety and embarrassing compulsions. I could be a kid again. Two years on, I slowly came off my medication. We waited, on edge, for symptoms to return, but they never did. I’ve often wondered why I never relapsed. It seemed impossible that something that had plagued me for so long had just vanished.
Thanks, PubMed
I wanted to know if other people had experiences similar to mine, so I headed over to trusty ol’ PubMed. I found several articles that explore the topic of OCD remission. Some have woefully small sample sizes and others are barely longitudinal, but there does seem to be a higher rate of OCD remission in the pediatric population than the adult population. The factors that influence this aren’t very well understood; some studies show that an earlier onset of symptoms predicts better outcomes, while others associate earlier onset with chronic, adult OCD. Don’t you just love conflicting results? I do, however, think these results can be reconciled.
Maybe It’s About Treatment, Not Age
A study published in 2014 followed up with children and adults with OCD over a three-year period. Children achieved remission more quickly than adults who had juvenile-onset of symptoms, but the age of onset did not affect the likelihood of remission. Instead, the authors show that the less time passes between the onset of symptoms and receiving treatment, the better the outcome.
This fits with the statistics on OCD treatment. In a different study by the same authors, children went an average of 1.5 years before receiving treatment, whereas adults reported a wide range of latency periods. On average, they went 14.5 years before receiving treatment, although the standard deviation was close to 12 years. Clearly, some adults suffer in silence for decades before getting treatment.
It’s plausible, then, that children who receive treatment soon after developing symptoms see remission more often, but children who endure a longer period of uninterrupted symptoms are more likely to have chronic OCD into adulthood.
The Takeaway
Multiple studies emphasized the importance of early recognition and treatment of childhood-onset OCD. Overall, I was encouraged by what I found during my deep dive into the literature. The sources I found all seemed to agree; long-term persistence of childhood-onset OCD is less common than it is for adult-onset OCD.
After all this, I’m still not sure whether I grew out of OCD. It’s difficult to determine whether anybody grows out of it without treatment because study samples come largely from inpatient and outpatient treatment centers. I will say that I occasionally get a sticky thought that reeks of OCD, but I set it aside fairly easily.
In a completely anecdotal way, this seems to me like the pathways that I was stuck in as a child had a chance to be rewired while I was on medication. Now, my brain can cope with intrusive thoughts pretty much like anybody else’s. If I had known that the chances were pretty good that I wouldn’t suffer from OCD forever, it might have been a little easier to cope as a child.
Treatment with ERP and medication offers adults and children relief from their OCD symptoms. So, if you have a kid with OCD, know that remission is possible. And for all the adults with OCD, know that there is hope, and you are not alone. Adults absolutely achieve remission as well. A 40-year follow-up study found that of 251 participants, improvement was observed in 83%. Those are pretty good odds!
A couple of years ago, my psych nurse suggested we send some of my cheek cells to a lab for genetic testing. I was severely depressed and hadn’t had much success with the antidepressants I’d tried. With a significant family history of depression and other mental health issues, it seemed likely that there was a genetic component for me.
My psych nurse told me that for some people, a genetic abnormality affects the activity of a particular enzyme that’s implicated in psychiatric conditions (and many other illnesses). People with this mutation can be helped by taking what’s essentially a supplement (I believe she even said it was “like a vitamin”), l-methylfolate. By taking the product of this hindered metabolic process in pill form, it fills in the gaps that your faulty enzymes have left behind. Because it was a rather serious situation, we decided that we may as well add this supplement to see if it helped. I told her I’d think about the genetic testing.
A couple of weeks later, we revisited the idea. The l-methylfolate seemed to be helping a little, but not dramatically. I had figured that the testing would be unnecessary; if the l-methylfolate helped, we’d know I was a mutant. If it didn’t, we’d move on to something else. It wasn’t that cut and dry.
Why the reluctance, you ask?
Perhaps there was a little anxiety about what I might find out about myself, but I suppose that’s a topic for my therapist. Mostly, I was skeptical. Genetic research has advanced tremendously, but the mechanistic aspects of mental illnesses are still rather poorly understood. Could a DNA profile really tell me why I was depressed?
Well, I’ll spoil the ending for you and say “Yes. Kind of.” Curiosity won out, and I agreed to part with some of my genetic material in the name of science and not wanting to be depressed forever. The results, pared down to what’s important for clinicians and patients to understand, were interesting- and rather ambiguous.
The science behind MTHFR mutations
The gene in question is called methylenetetrahydrofolate reductase (MTHFR). Our genes code for proteins, and enzymes like MTHFR are one type of protein. MTHFR is involved in something called one-carbon metabolism, which has effects on the production of neurotransmitters.
First, some genetics background
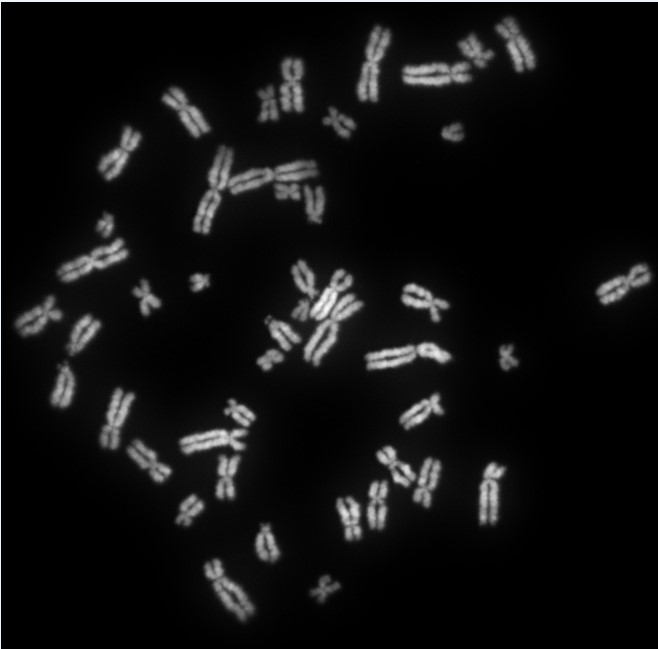
Harken back to your high school or college biology class; remember alleles? A gene and an allele are not exactly the same thing. A gene is essentially a small segment of a chromosome. The DNA sequence of a gene codes for a specific sequence of amino acids, which comprise proteins. An allele, however, is a variation of a gene. For each gene, you got one allele from your mom and one from your dad. I received a combination of normal and mutated MTHFR genes. Mutation is how variation occurs, and the process itself is neither good nor bad; it just is. Some mutations are adaptive, some are neutral, and some are deleterious.
Two MTHFR mutations
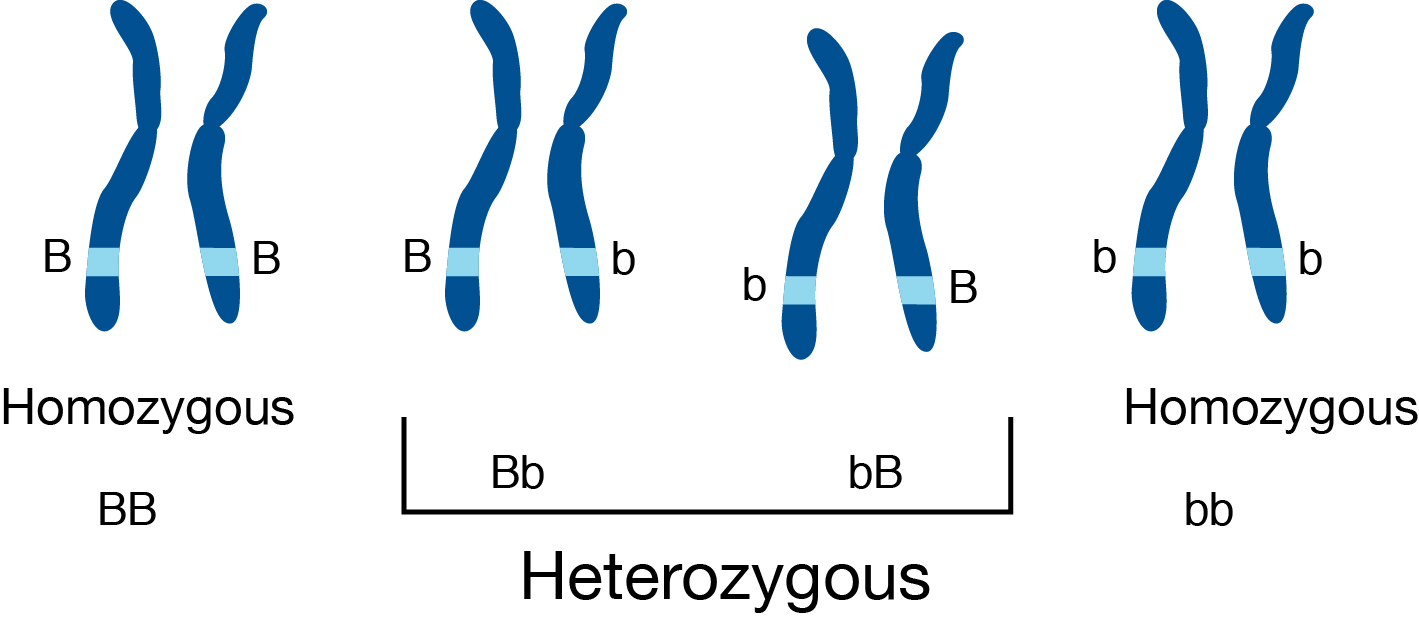
There are two main mutations on the same allele that seem to affect this enzyme’s activity. As usual, the names are cryptic; they’re called C677T and A1298C. The numbers and letters refer to where in the allele one nucleotide (or one “digit” in the DNA code) has been changed to another, and the substitution that’s taken place. In general genetics contexts, heterozygotes have different alleles from mom and dad, while homozygotes have identical alleles.
In the context of mutation research, there is typically one genotype that is referred to as “wild type,” meaning it contains no mutations and has full function. In this case, imagine the big “B” homozygous chromosome in the image above as the “wild type” and the little “b” as the mutation in question. The letters in examples like this are simply ways to represent alleles in a theoretical framework. The order of the letters is written out because, without further research, it’s difficult to tell which parent the mutation came from.
To bring it around to MTHFR, I’m a heterozygote for both of the main mutations (this is called “compound heterozygosity”). My genotype for C677T is C/T. The C (cytosine) is the nucleotide in the normal allele and the T (thymine) is the substituted nucleotide in my mutated version. I got the C from one parent and the T from the other. I’m also a heterozygote when it comes to the A1298C mutation. My genotype is A/C, where the A (adenosine) is the normal one and the C is the mutant.
The problem lies in the metabolism of a key metabolic precursor: a biologically-active form of folate. The product of this reaction is 5-tetrahydrofolate, which provides a methyl group for epigenetic regulation. In other words, when MTHFR is mutated, the system that controls gene expression and, ultimately, neurotransmitter production, is affected by a lack of this enzyme’s product because the enzyme’s function is reduced. This is the gap that the supplement I take fills in.
Enzyme activity
Meta-analyses suggest that C677T homozygous mutants (they have two mutated copies) have a 75% reduction in MTHFR activity, and A1298C homozygous mutants have a 39% reduction in enzyme activity. Heterozygotes for each mutation have less severe reductions in activity, but if you’re a compound heterozygote (like me), that results in a 52% reduction. So, I have slightly less than half the enzymatic activity for MTHFR than a normal, non-mutant.
MTHFR and depression
That all seems pretty straightforward, but take a look at the plethora of studies that exist on the internet, and you’ll see why I was cautious. Some have found significant relationships between MTHFR polymorphisms and psychiatric conditions, and yet others haven’t. There are some studies that say that there is no difference between mutant and control subjects when it comes to depression. Others suggest that carrying a mutated MTHFR allele predicts depression when the person is exposed to childhood trauma.
The consensus seems to be that more research is needed, although increasingly, there does seem to be a relationship between MTHFR and depression.
For me, I’m content to believe that at least some of my struggles can be traced back to MTHFR. The supplement does seem to make my antidepressants more effective. Plus, that’s not all that my genetic report showed. I also have a weird serotonin transporter that makes SSRIs less effective and increases my cortisol release in response to stress. I’m glad I did the test, at the very least because it helped me to accept my disorder as valid and offered insights into my mental health..
The future of mental health treatment
Is this a sure-fire way to treat mental illness? I’d say not yet, but it’s certainly valuable. Personalized medicine seems to be a buzzword floating around these days, and the implications of genetic research for how we approach mental illness are fascinating. Maybe when the relationships between genes and mental illness are elucidated a little more clearly, we can finally kick the stigma and misconceptions out the door. One can hope, at least.

 It’s nothing to be ashamed of I tell myself twice daily. What day is it? They all blend together. I open the third compartment, pour the pills into my palm, wait for a moment. Maybe this day will be the day. Maybe if I give the medicine a moment of silence; infuse it with my desperation before I let it fall down the dark well of my esophagus.
It’s nothing to be ashamed of I tell myself twice daily. What day is it? They all blend together. I open the third compartment, pour the pills into my palm, wait for a moment. Maybe this day will be the day. Maybe if I give the medicine a moment of silence; infuse it with my desperation before I let it fall down the dark well of my esophagus.