You would think I had learned my lesson. Refilling my medicines is not something I find easy to do if a phone call is involved. I waited until the very end of my supply to refill my Deplin, and now, because of shipping delays, I’ve been without for several days. Deplin contains l-methylfolate, which fills a metabolic gap caused by a mutation in the MTHFR gene. Essentially, it helps my antidepressant work. Not taking my Deplin is what pushed my suicidality to new lows last year when I was hospitalized. It seems like I can feel my brain slowing down. I sleep all day like I’m hibernating in reverse by starting in spring. There is nothing to get me up except the dog, who stands by my bed and huffs at me, threatening to wake me with a full bark if I do not move. I accomplish the necessary and return to bed, already sinking into sleep. The occasional diversion brings some welcome entertainment, but it’s just a momentary distraction.
Me. It’s me. (Unsplash user @successfullycanadian)
I took some time off of work when my grandfather passed away last week, but then I decided it would be more helpful to have something to do. So, I went back to work (which I thankfully do from home under normal circumstances) on Monday. Unfortunately, it’s shaping up to be a slow week, anyway. I suppose I should turn to hobbies to fill my time. I’m partway through a drawing that I promised to someone, but like many of us judging ourselves for not utilizing all of this time to finish household projects or write a sonnet or whatever we think we should be doing, motivation eludes me.
My shipment of Deplin is finally at my local post office and should be delivered by the end of the day today. It couldn’t come too soon. I plan to rip it open right there at the mailbox and throw one down the hatch. Well, okay, maybe I’ll go inside for a glass of water.
I’d like to introduce you to my irrational brain, partly to illustrate how distorted depression can make your thoughts, and partly to convince myself that this will pass. I take methylfolate because I’m a mutant and it helps my antidepressants work better. I ran out a couple of weeks ago and was slow to get it refilled. There aren’t any withdrawal symptoms of going cold-turkey because it’s really more of a supplement than anything else. (I’m much more careful about my other medications; you should never stop taking antidepressants suddenly without the supervision of your doctor.)
In any case, I didn’t call right away to get my methylfolate refilled. Initially, I thought that it would surely stay in my system for a few days and that it wouldn’t be a big deal to go without it briefly. In hindsight, that was a mistake. It was ok for a few days, but once I started to feel my depression worsen, I started to think some really unhelpful thoughts.
I messed up by not being on top of my responsibilities health-wise. This is my fault. I deserve to feel this. Therefore, I should not refill this medication, so as to prolong my suffering and punish myself.
Uh, no. Just… no. This is rational brain speaking. The statements above are utter nonsense and are not helpful in the slightest.
While I know that the most logical explanation for this decline in my mood is the lack of that medication, irrational brain whispers that maybe it’s just me. And that just in case it’s not me, and the arrival of that medication marks an end to this little blip, now’s my chance to self-destruct.
Seriously. Where do these thoughts come from?! Here’s another example: I was sitting outside with my dog and realized I hadn’t had any water in a while. Out of nowhere, my irrational, depressed brain said I deserve to be thirsty.
Apparently, I should just completely deprive myself of all comfort and nourishment, because according to my automatic thoughts, I’m a terrible person.
My meds have arrived, so the thing to do now is to try not to listen to myself until they kick in. Much easier said than done. In the meantime, I’m doing my best. That’s all we can ever do.
A couple of years ago, my psych nurse suggested we send some of my cheek cells to a lab for genetic testing. I was severely depressed and hadn’t had much success with the antidepressants I’d tried. With a significant family history of depression and other mental health issues, it seemed likely that there was a genetic component for me.
My psych nurse told me that for some people, a genetic abnormality affects the activity of a particular enzyme that’s implicated in psychiatric conditions (and many other illnesses). People with this mutation can be helped by taking what’s essentially a supplement (I believe she even said it was “like a vitamin”), l-methylfolate. By taking the product of this hindered metabolic process in pill form, it fills in the gaps that your faulty enzymes have left behind. Because it was a rather serious situation, we decided that we may as well add this supplement to see if it helped. I told her I’d think about the genetic testing.
A couple of weeks later, we revisited the idea. The l-methylfolate seemed to be helping a little, but not dramatically. I had figured that the testing would be unnecessary; if the l-methylfolate helped, we’d know I was a mutant. If it didn’t, we’d move on to something else. It wasn’t that cut and dry.
Why the reluctance, you ask?
Perhaps there was a little anxiety about what I might find out about myself, but I suppose that’s a topic for my therapist. Mostly, I was skeptical. Genetic research has advanced tremendously, but the mechanistic aspects of mental illnesses are still rather poorly understood. Could a DNA profile really tell me why I was depressed?
Well, I’ll spoil the ending for you and say “Yes. Kind of.” Curiosity won out, and I agreed to part with some of my genetic material in the name of science and not wanting to be depressed forever. The results, pared down to what’s important for clinicians and patients to understand, were interesting- and rather ambiguous.
The science behind MTHFR mutations
The gene in question is called methylenetetrahydrofolate reductase (MTHFR). Our genes code for proteins, and enzymes like MTHFR are one type of protein. MTHFR is involved in something called one-carbon metabolism, which has effects on the production of neurotransmitters.
First, some genetics background
Harken back to your high school or college biology class; remember alleles? A gene and an allele are not exactly the same thing. A gene is essentially a small segment of a chromosome. The DNA sequence of a gene codes for a specific sequence of amino acids, which comprise proteins. An allele, however, is a variation of a gene. For each gene, you got one allele from your mom and one from your dad. I received a combination of normal and mutated MTHFR genes. Mutation is how variation occurs, and the process itself is neither good nor bad; it just is. Some mutations are adaptive, some are neutral, and some are deleterious.
Two MTHFR mutations
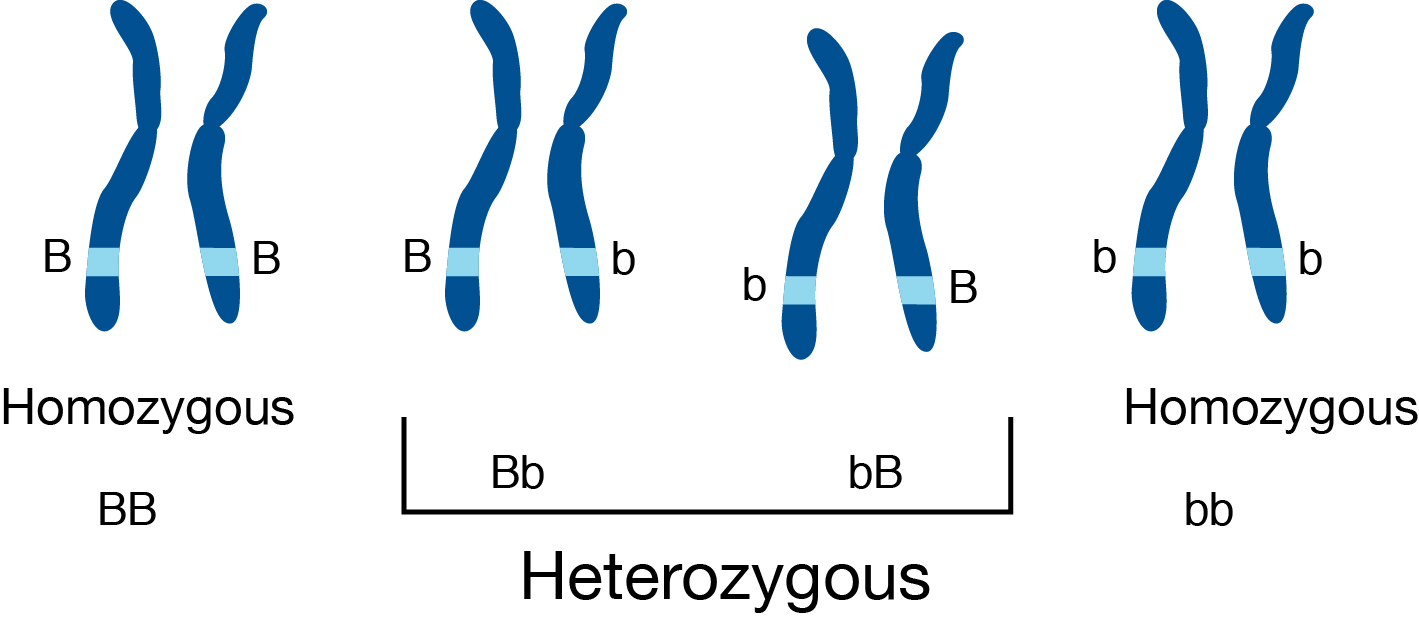
There are two main mutations on the same allele that seem to affect this enzyme’s activity. As usual, the names are cryptic; they’re called C677T and A1298C. The numbers and letters refer to where in the allele one nucleotide (or one “digit” in the DNA code) has been changed to another, and the substitution that’s taken place. In general genetics contexts, heterozygotes have different alleles from mom and dad, while homozygotes have identical alleles.
In the context of mutation research, there is typically one genotype that is referred to as “wild type,” meaning it contains no mutations and has full function. In this case, imagine the big “B” homozygous chromosome in the image above as the “wild type” and the little “b” as the mutation in question. The letters in examples like this are simply ways to represent alleles in a theoretical framework. The order of the letters is written out because, without further research, it’s difficult to tell which parent the mutation came from.
To bring it around to MTHFR, I’m a heterozygote for both of the main mutations (this is called “compound heterozygosity”). My genotype for C677T is C/T. The C (cytosine) is the nucleotide in the normal allele and the T (thymine) is the substituted nucleotide in my mutated version. I got the C from one parent and the T from the other. I’m also a heterozygote when it comes to the A1298C mutation. My genotype is A/C, where the A (adenosine) is the normal one and the C is the mutant.
The problem lies in the metabolism of a key metabolic precursor: a biologically-active form of folate. The product of this reaction is 5-tetrahydrofolate, which provides a methyl group for epigenetic regulation. In other words, when MTHFR is mutated, the system that controls gene expression and, ultimately, neurotransmitter production, is affected by a lack of this enzyme’s product because the enzyme’s function is reduced. This is the gap that the supplement I take fills in.
Enzyme activity
Meta-analyses suggest that C677T homozygous mutants (they have two mutated copies) have a 75% reduction in MTHFR activity, and A1298C homozygous mutants have a 39% reduction in enzyme activity. Heterozygotes for each mutation have less severe reductions in activity, but if you’re a compound heterozygote (like me), that results in a 52% reduction. So, I have slightly less than half the enzymatic activity for MTHFR than a normal, non-mutant.
MTHFR and depression
That all seems pretty straightforward, but take a look at the plethora of studies that exist on the internet, and you’ll see why I was cautious. Some have found significant relationships between MTHFR polymorphisms and psychiatric conditions, and yet others haven’t. There are some studies that say that there is no difference between mutant and control subjects when it comes to depression. Others suggest that carrying a mutated MTHFR allele predicts depression when the person is exposed to childhood trauma.
The consensus seems to be that more research is needed, although increasingly, there does seem to be a relationship between MTHFR and depression.
For me, I’m content to believe that at least some of my struggles can be traced back to MTHFR. The supplement does seem to make my antidepressants more effective. Plus, that’s not all that my genetic report showed. I also have a weird serotonin transporter that makes SSRIs less effective and increases my cortisol release in response to stress. I’m glad I did the test, at the very least because it helped me to accept my disorder as valid and offered insights into my mental health..
The future of mental health treatment
Is this a sure-fire way to treat mental illness? I’d say not yet, but it’s certainly valuable. Personalized medicine seems to be a buzzword floating around these days, and the implications of genetic research for how we approach mental illness are fascinating. Maybe when the relationships between genes and mental illness are elucidated a little more clearly, we can finally kick the stigma and misconceptions out the door. One can hope, at least.