If you’ve been keeping up with my posts lately, you know that I’ve been having a rough time of things. I’m waiting for my new medication to kick in and doing my best to implement skills I’m learning in partial hospitalization. Whether it’s the meds, the skills, or just the ebb and flow of emotion, I’m finding myself…feeling….feelings. Wild, right?! The numbness is retreating and being replaced with actual emotions. Which, is good. I think. I’m no longer feeling crushing sadness through a thick haze of nothingness; I’m feeling crushing sadness in a pure, unadulterated manner. But, that’s okay- because it passes. I’m trying to work on my mindfulness skills. The sadness checks in, I sit with it and do my best not to catastrophize that it will stay forever, then my dog does something funny and amusement bumps the sadness out of the way.
Later, I’m outside, enjoying the sunshine when sadness saunters up again and says “Hey. Really sucks that you missed out on all of this pleasantness when you were in bed for days on end, doesn’t it?” Yeah. Yeah, it does. Thanks for that reminder, brain. So then I’m sad about being sad. I’m meta sad. Immediately, worry and despair pop in to let me know that a moment of enjoyment doesn’t fix everything and that I still have a long way to go. Oops, now I’m crying, and maybe I’ve ruined the moment entirely. Quick, focus on the sunshine! Focus.On the. Dandelions!
Forcing yourself to be mindful is kind of the opposite of mindfulness. Clearly, I have some work to do, which is why this weekend I’m trying to embrace the “non-judgmental” part of mindfulness. Emotions are healthy, and although I’m still feeling more negative ones than I’d like to, it’s ok that they’re there. When I start to feel sad about the past or anxious about the future, the best way to not get trapped in it is to just notice it and then redirect my thoughts. The weather is beautiful, I’m fortunate in more ways than I can count, and it’s ok to take time to heal.
They thanked me for my vulnerability, but it spilled out by accident, like beads of condensed sadness crammed into a too-small vessel. A wave comes, and while I sit among this circle of strangers, I cry. Nine sad faces avert their eyes. Is this circle a liferaft or a sinkhole?
In the distance, we see life as it should be- a mental ecosystem in balance. For six hours each day, we hover on the edges of the ring, tossing insecurities, worries, and vulnerabilities into the middle. We wait to see if they sink, but often, they float back to us. At three P.M., we depart; a snippet of normal routine, just long enough for our symptoms to impair us under the cover of darkness, then it’s back to the circle again. Soon, each of us will leave and swim to shore, but for now, we are lost at sea. All we can do is embrace our vulnerability and let it carry us towards one another.
Last week, I was discharged from an 11 day stay in a psychiatric hospital. This week, I spent six hours every day in a partial hospitalization program. Since being admitted almost three weeks ago, I’ve received more messages of concern and support than I know how to process, and that’s a little bit scary.
A part of me is resistant to receiving so much love because it means that all of these people know about a part of my life that contains a good deal of shame. My instinct is to politely accept the well-wishes and then quietly close the door and never discuss it again. Unfortunately, being independent to a fault can get you in trouble. It can make you more likely to wait too long to ask for help, at which point, the situation has snowballed out of control and it’s a crisis. So, reach out to your loved ones. Ask for help and offer help. Being vulnerable is how we connect.
I spent a week and a half hospitalized for depression as an inpatient at a behavioral health hospital, and all I got was a lot of decaf, terrible antiperspirant, and ungroomed eyebrows (dangerously close to being “eyebrow”). Oh, and a will to live.
When I ran out of methylfolate, my mutant brain began to rebel. All of the work I had done to pull myself out of the dark pit of depression flew out the window as my symptoms came roaring back. I was tired of living with the darkness, the fatigue, the brain fog, and the sadness of depression. And, because it seemed that there was no other way to live, I was tired of living. I fell into the old habits of isolating, harming myself, and outwardly presenting as if everything were fine.
When you stuff everything down, at some point you run out of space. My tipping point came during my weekly therapy session. After describing the hopelessness and elaborating on the details of my thoughts about suicide, my therapist convinced me to go to the hospital. Once I had been assessed, I was given the choice (that wasn’t really a choice) to either sign myself in voluntarily or be put on a 72-hour hold. I signed myself in.
The unit I was on is designed to be a crisis stabilization unit. There’s no one-on-one therapy, visiting hours are actually a singular visiting hour each day, and the items you’re allowed to have are extremely limited. Patients are expected to be in group therapy, meeting with a doctor or social worker, or working on an alternate activity like journaling. You are locked out of your bedroom for most of the day, so your options for privacy are slim to none. You and your roommate must sleep with the door open, as nurses walk around all night long doing “checks,” where they mark down your whereabouts and what you’re doing on their clipboard paperwork. Not to mention your bed is hard and noisy, and your pillow feels like a sack of uncooked rice. It was a difficult environment to be in for 11 days, to say the least.
Being hospitalized for depression is not easy, but the good news is, it works. I switched medications, and while it’s too soon to say whether it’s a good fit for me, being kept in a safe place surrounded by people who understood what I was going through went a long way towards getting me back on my feet. The groups tended to cover topics that were familiar to me, so not much of the information was new. That being said, hearing other patients’ perspectives and experiences was what made my stay helpful.
I stayed for several days longer than the average at that hospital. The staff wanted to see more improvement than I was making, and I wanted to avoid triggering a 72-hour hold by declaring that I was checking out against medical advice. This resulted in my estimated discharge date being pushed out a day or two at a time while my frustration levels grew. Eventually, I agreed to do a partial hospitalization program at a different facility near where I live. This was enough to convince the staff that I was safe to go home. Today, I start the process of doing a PHP. I feel much better than I did when I was admitted to the hospital. I know that shifting back into my normal routines will be a tricky transition and that a week and a half in a hospital doesn’t fix everything. But, it’s a start.
We all have those sneaky thoughts that come unbidden when we make a mistake or are faced with a change. I don’t know a single person who hasn’t mentally beat themselves up over a perceived shortcoming. Often, it isn’t deserved. But when your automatic thoughts are that you deserve those thoughts, what do you do?
“Automaticity is granted if the perceiver lacks awareness of the process, does it with efficiency (i.e., with minimal use of cognitive resources), has no intention to do it, or cannot control it.”
Based on this definition, automatic thoughts include those about others, such as deeply held prejudices. It also includes the intrusive thoughts that characterize Obsessive Compulsive Disorder, but I’ll be focusing more on those automatic thoughts that don’t necessarily play a direct role in psychopathology. For example, self-referential thoughts like, “I’m going to fail this exam. I always fail.” Those are the types of thoughts I’m talking about here.
Negative Automatic Thoughts
The most well-known measure in this area is the Automatic Thoughts Questionnaire (ATQ), a 30-item instrument developed in 1980. The ATQ contains statements like “I am a failure,” and asks participants to rate each statement on a scale representing the frequency with which they experience that thought. It’s a cross-validated questionnaire that’s been shown in several studies to correlate with depression and separate depressed from non-depressed individuals.
When presented with a distressing stimulus, previously depressed participants and people who have never been depressed experienced stronger belief in negative automatic thoughts. The researchers propose that cognitive reactivity is related to relapse and recurrence of depression.
Cognitive reactivity refers to the triggering of negative thought patterns by small declines in mood. The ability to resist slipping into negative cognitions seems to have a protective effect; inpatient surveys taken at two time points show that decreases in negative automatic thoughts are strongly correlated with reduced suicidal ideation.
Positive Automatic Thoughts
The relationship between negative automatic thoughts and depression and anxiety is well documented. We can infer that the lackof negative automatic thoughts has beneficial effects on mental health, but this still isn’t quite the same as the presence of positive automatic thoughts. However, research does support the assumption that positive thinking is related to positive mood. A variation of the ATQ was developed to measure positive automatic thoughts. It’s called the ATQ-P, and higher scores on it are strongly associated with lower levels of depression. A healthy balance of positive and negative thoughts appears to be weighted toward more positive than negative- a ratio of 0.62 to 0.38, to be exact (according to one study).
Where Exactly Do Automatic Thoughts Come From?
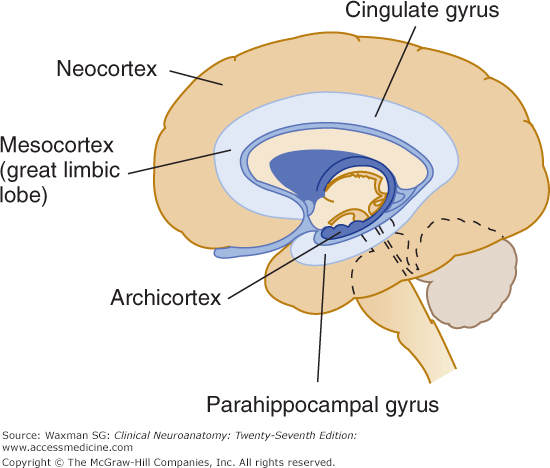
Parahippocampal gyrus
One area of the brain that is linked to automatic thoughts is the parahippocampal gyrus, a part of the limbic system.
“The voxel-based morphometry results showed that the GMV of the right parahippocampal gyrus and fusiform gyrus and the WMV of the right superior temporal pole increased with the severity of depression.”
Let’s break that down. A voxel is a value assigned to a three-dimensional grid. Think “pixel” but with volume. Voxel-based morphometry is a technique for assessing differences in brain volume. Brain scans are registered to a standard, voxel-based template, then each voxel is “smoothed” by averaging it with the values of the surrounding voxels. Finally, the image volume of each scan is compared to the other scans’ volumes and the differences between voxels are evaluated statistically. Basically, it’s a way to quickly compare lots of structural brain scans using computers.
The study found that increases in the volume of grey and white matter in certain regions of the limbic system are associated with increasing severity of depression, as measured with the ATQ. So, negative automatic thoughts are associated with depression, and depression is associated with higher volume in the emotional center of the brain. That doesn’t necessarily mean that negative automatic thoughts are directly related to grey and white matter volume. Or does it?
Statistical tests showed that the combination of automatic thoughts and grey matter volume in the parahippocampal gyrus predicted depression measured by the ATQ and the Self-Rating Depression Scale. The automatic thoughts mediate the relationship between volume and depression. They also seem to mediate the relationship between neuroticism and depression.
Medial Prefrontal Cortex
The medial prefrontal cortex is not part of the limbic system. It’s located at the very front of your brain and is associated with the processing of social information. Hyperactivity in this region has been linked to neuroticism and self-generated thought. The tendency to worry and impose self-generated beliefs onto a reality that doesn’t match those beliefs sounds a lot like the automatic thoughts in the studies above. But it’s not all bad; the same hyperactivity and self-generated thoughts are also associated with creativity.
Combatting Negative Automatic Thoughts
Hopefully, you haven’t read all of that and decided that the next time someone tells you to be more positive you’ll just say “the grey matter in my parahippocampal gyrus says, ‘No can do.'”
Photo by @linkedinsalesnavigator on Unsplash
Cognitive behavioral therapy has been shown to result in reductions of automatic thoughts and dysfunctional attitudes associated with non-clinical depression. CBT makes use of behavioral experiments and automatic thought records. People perceive behavioral experiments to be more powerful than combatting automatic thoughts with logic alone, which could be because behavioral experiments function through emotion-based cognitive systems. Mindfulness has also been shown to reduce automatic thoughts, and it’s associated with increased life satisfaction.
There are plenty of reasons to believe that we have the power to effect change in our own brains.
What helps you recognize negative automatic thoughts, and how do you practice self-compassion?
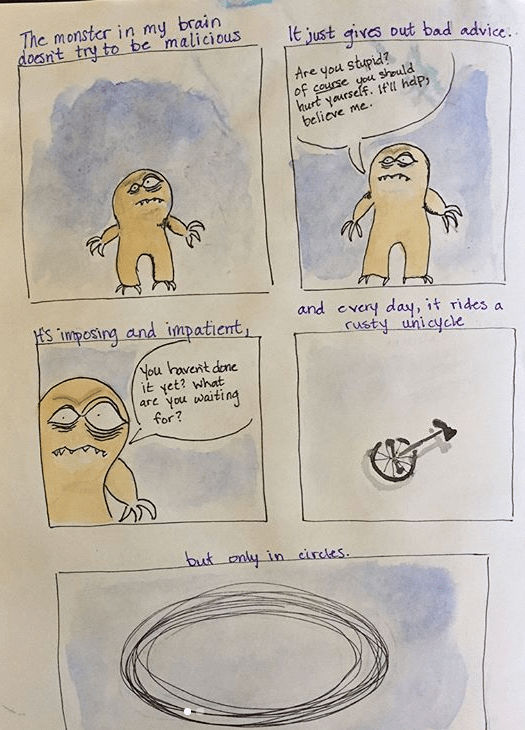
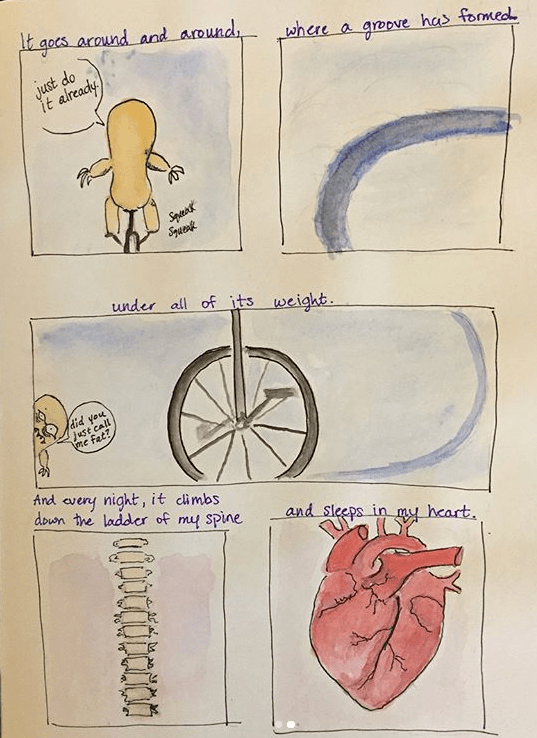
What is a lumpdate? I’m glad you asked. “The Lump” is the name I use to refer to the imaginary goblin in my brain that rides a tiny, rusty unicycle in circles, day and night.
The Lump was quiet for a while, but it’s back again, so this is a lumpdate- an update about the Lump. It won’t be a long lumpdate; the Lump is rather unoriginal and doesn’t have many new points to make. Really, they’re all repeats of the same damaging doubts from before.
In sum, the Lump is back, setting up shop in my mind.