I’m prone to an almost crippling inability to verbalize my feelings. Some of that is because of Sensory Processing Disorder, and some is probably due to depression and other factors, like my need to feel capable and independent, which results in me pretending I have no feelings whatsoever and consequently getting no practice in identifying them, but the point is: metaphors. I love ’em.
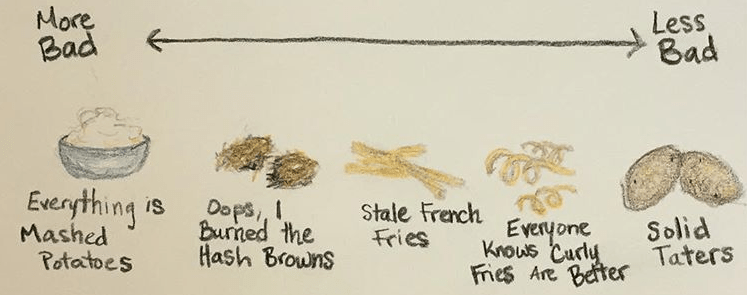
For inexplicable reasons, I find it so much easier to say “everything is mashed potatoes” than to say “I’m lost in a miserable fog of depression.” (Actually, come to think of it, that second one is also a metaphor, but you get the idea.) Hence: The Potato Scale of Depression.
It’s Not a Good Scale (but it kind of is)
Roughly ten months ago, I really did tell my friends “everything is mashed potatoes,” and thus, The Scale was born. Unlike other scales, there are no numbers, no frowny faces, and no defined increments between items. In other words, it’s a terrible scale. There’s no way to objectively determine how someone is feeling based on the potato scale of depression, but it worked for me during a time when talking about my feelings was both very difficult and very important. It became a kind of inside joke, and my friends would ask me “how are the taters?” and I’d respond with some arbitrary, starchy answer:
“Tots,” or “potato pancakes,” or “undercooked hash browns,” or “just the eyes.”
They’re all utterly meaningless answers, but they started a conversation. We’d debate the relative positive and negative qualities of each dish, and it served (pun intended) to connect us when all I wanted to do was withdraw.
Laughter = The Okayest Medicine
Eventually, I became more comfortable with talking about my emotions. A silly scale opened the door (metaphors are everywhere) to talking about how I really feel. Sometimes using humor to defuse stressful situations and topics gets a bad rap, but it’s incredibly common. Plus, research shows that the right kind of humor can have a protective effect against recurring depression. The adaptive forms of humor (self-enhancing and affiliative) are associated with emotion regulation and positive mental health. The maladaptive forms of humor are the aggressive and self-defeating types. I could probably dedicate an entire post to why I think suicide jokes aren’t funny or healthy, but this is a post about a nonsensical tuber scale. So- perhaps another time. Back to the adaptive humor:
In consequence, an individual can successfully distance himself/herself from a negative situation and appraise its meaning from a less distressing point of view.
When you mentally distance yourself from a negative situation, you’re creating what researchers call “metacognitive awareness,” where thoughts and behaviors are interpreted as “mental events, rather than as the self.” Mental illnesses can often be associated with feelings of guilt and inadequacy, which is why it’s important to take a step back and remember that your symptoms are not character flaws. This has become a regular mantra for me, and anytime I start thinking badly of myself for my symptoms, I turn it around with I’m not lazy, I’m just soggy hashbrowns right now. Y’know, the kind that maybe didn’t get cooked enough, so now they’re getting cold and seeping oil onto your toast. Depending on your humor preferences, this might border on maladaptive, but it reminds me to not get bogged down in a temporary feeling or judgment. And really, what potato dish isn’t still delicious, no matter how poorly cooked?
Depression Scales: PHQ9, Who?
The Potato Scale of Depression is obviously not a tool that will ever be used in any kind of professional setting, but that doesn’t mean that it can’t be beneficial. Maybe potatoes aren’t your thing, and some other metaphor would be more helpful. Whatever it is, I know that for me, finding a less clinical way to communicate how I feel has made it way easier to do so.
May you all have curly fries and solid taters for the foreseeable future.
2021 Update: My therapist and I now have a wide repertoire of replacement metaphors, including “clams” in place of “goals” and “feathers” in place of “small barriers between inaction and action.” The Potato Scale of Depression has fallen to the wayside, likely because I have gotten better at saying words about how I feel. Therapy works!