There is no sleep like the sleep of parched eyelids and lithium limbs. Even before you swallow your nightly dose, your breathing deepens, your spine curves forward. Your thoughts retreat to a distant rumble, as if your brain is hosting a party to which you weren’t invited. Perhaps you’re already asleep. Maybe. Did you ever wake up? Maybe not.
In the morning, you place more pills on your tongue and let them be carried down with the water your kidneys are begging for. Today, you tell yourself, no more sleep. I have things to do. But then it’s only been three hours since you rose this morning, and you find yourself sitting heavy on your bed, quickly slipping into the horizontal. No! No more sleep. You drag yourself from your cozy nest and plod to a less comfortable seat.
Yesterday, you slept for four and a half hours in the afternoon, and at that point, is it even called a nap? That’s just second bedtime in your book. And so today, like all the other days, you vow no more sleep. But your bed has its own gravity just for you, and before long, you’re crawling in; a perfect cove, with blanket waves and a pillow beach. Through the open window, you can almost taste the breeze, laden with lithium salt.
Love,
Your brain
I should be clear. I’ve been plagued by suicidal thoughts for three years, sometimes worse than others. Taking a high dose of lithium has given me, by far, the most dramatic positive result of any medication I’ve taken in my adult life.
I don’t want this post to be just another internet story about how terrible a particular psychiatric medicine was for someone. Those reviews are usually written by the people who had the worst side effects and the least benefit; after all, they’re the most motivated to write a review. Every medication has benefits and drawbacks. Scrolling through pages and pages of negative experiences paints a picture that doesn’t capture the thousands of people whose lives are vastly improved by that medicine.
It’s not perfect, and I still have bad days. It’s also a possibility that these sleep marathons are partly a symptom of my depression or the combination of meds I take that can make you drowsy. While I hope that lithium is not a medication I have to take long-term, I would be remiss if I didn’t acknowledge that taking it has probably saved my life.
In the depths of depression and throughout the hills and dips of recovery, apathy is a frequent visitor. It steals motivation and leaves nothing behind. When this happens, it’s tempting to let it overtake you. I’ve found that continuing with a task despite apathy can help end a spell of it. Here are some of the ways I use to get me through a period of apathy.
Rewards
Whatever gets you even a little bit motivated can be useful when battling apathy. Granted, if you’re feeling apathetic, even the usual rewards might not have much of an effect. For me, I sit in the shade with a book and my dog. Maybe for you, it’s watching your favorite show or treating yourself to a delicious snack. Whatever it is, reward yourself for your hard work; apathy isn’t easy to overcome.
A Conversation With Future You
You might not care right now, but you might care a lot in the future. We like to think that we can predict the future, but the truth is that none of us really know what’s going to happen in a week or a month or a year. So, while this one requires a little hope for the future, sometimes all it takes is to allow for the possibility that things might get better; to admit that you’re not a fortune-teller. In fact, I’m working on this one right now.
Cultivate Satisfaction
I know what you’re thinking–well, I don’t know. (That’s another distortion.) But you might be thinking “obviously, if I’m feeling apathetic, I don’t want to do anything because I don’t get satisfaction from completing a task. Why would I do something that gives me no intrinsic reward?”
Well, that’s a good point. I’ll counter with this: an oyster creates a pearl when a grain of sand becomes lodged in its tissues. Layer by layer, the mollusk coats the grain of sand with calcium carbonate to protect itself from the irritating particle. What began as a negative from the oyster’s perspective is turned into something valuable.
Motivation often comes from the desire to solve a problem. Whether it’s a seemingly small problem like noticing that your hair needs to be washed, or a larger-scale problem like slipping grades that could affect your graduation, everything we do, we do to solve a problem. Every time you do something that moves you towards a goal, you’re building a metaphorical layer around the underlying issue. Every time you go to class even though you don’t want to, you’re building up to something great. Every time you go for a run even though you’d rather sleep, you add another layer of persistence to your pearl.
Often, it’s only after many layers, many instances of forcing myself through apathy, that I begin to get a glimmer of satisfaction. Sometimes, the only way to reach the other side of apathy is to just begin. Momentum only comes when you start to move.
Lately, I’ve been noticing the return of one of my most distressing depression symptoms: thoughts about self-harm. When I first started harming myself, I was so ashamed that I couldn’t talk about it at all. When asked, I’d shut down and say nothing for fear of crying uncontrollably. I have the same struggle when it comes to suicidal ideation; I feel such overwhelming shame that just saying the words out loud has been a gradual process. I was recently talking to my (very patient) nurse practitioner, who reminded me that the first time we talked about my suicidal thoughts it took me about ten minutes to get the words out, and I was shaking like a leaf the whole time.
It’s only recently that I’ve really been working on seeing these things – self-harm and suicidal thoughts – for what they are: symptoms of a larger issue. They’re indicators that my depression has worsened. There should be no judgments about willpower or self-control. They’re symptoms that should be taken seriously, but they’re nothing more or less – just symptoms.
While I know this intellectually, when those old thoughts come rushing back, so do the remnants of guilt and shame that I’ve worked to eliminate. It eats at me – the thoughts themselves and the judgments I hold against them. That’s how it always is; whether it’s a trickle or a flood, the thoughts eventually erode my determination not to give in to self-harm. It’s a battle to hold out until the thoughts pass, and sometimes I make it, but sometimes I don’t. The good news is, it does get easier with time and practice. If you relapse it can feel like you’re back at square one, but you’re not. If you need a little encouragement today, keep going. Keep working to treat yourself with kindness. You’ve got this.
A short drive up a dirt road after a long drive up a canyon, there is a cabin in the woods. Inside, there is a sleeping dog–wearing her coat of all-black fur, resting on her side, one upright ear has flopped over. She has sniffed every inch of this cabin since we arrived yesterday afternoon. Her job complete for now, she allows herself a brief intermission to do what puppies do– nap soundly and sweetly.
I am sitting in an armchair near the sleeping dog. I came to the cabin for a short reprieve, to escape the relentless tide of life’s obligations. Most of them, I left behind. But one, I can’t seem to shake. A black dog followed me up here, and not the one at my feet. It goes where I go, does what I do. It can be menacing and imposing, or familiar and safe. This black dog is of my brain’s own creation, made from worry and sadness and guilt. It was set in motion before I knew of its existence. It came from faulty neurotransmitters, genetic predispositions, and the fickle imaginings of chance.
The black dog at my feet jolts awake — a noise on the stairs. It is only the cabin creaking, so she returns to her slumber. We both settle into the peaceful sounds of the woods. A duck laughs on the pond. Swallows swoop and chirp over the water, plucking mosquitos from the sky. A gurgling brook feeds the pond, and its sound is a balm to a worn-out mind. But a balm cannot evict the black dog of depression. It howls its objection, then herds me back to bed, nipping my heels with fatigue and foggy thoughts. As I sink into sleep, I know that soon, my other black dog will come to wake me. She will breathe on my face and wag her tail. She will tell me that it’s time to get up, time to go out, time to take in the sounds and smells of this short reprieve in the woods.
I have an appointment coming up with my psychiatric nurse practitioner, and that means my thoughts frequently settle on the effectiveness of my mental health treatment. By now, I’m familiar with the questions she’ll likely ask me, but somehow the answers never come easily. Determining how I feel is not something I’m very good at, although I’ve gotten better at it. This time, I’ll attempt to describe the seemingly endless plateau of “meh” on which my mood currently resides. I have occasional dips into the dark chasm of “really bad,” but for the most part, things are ok. But as I decided after I was released from the hospital, I’m not settling for “ok” this time. I want to feel great, exuberant, joyful, even- happy. Happy would be good.
At this point, it seems like I’m running out of viable mental health treatment options that come in pill form. I was told I was a candidate for and encouraged to try Electroconvulsive Therapy (ECT) while in the hospital (a treatment that has changed immensely since it first began). My mother’s worried googling turned up IV ketamine as a promising treatment that my psych NP also encouraged. I knew people in my partial hospitalization program that moved on to do Transcranial Magnetic Stimulation (TMS). These are all safe treatments that, if they work, can change your life for the better. So, why am I so resistant to the idea?
I think it comes down to acceptance. When I first became depressed, it took me a long time to get to a place where I felt comfortable taking antidepressants. I clung to (and sometimes still do) the idea that if I just tried harder, all my problems would be solved. This is because, like many of us, I’m way too hard on myself. But it’s also because it was scary to fully accept that I have an illness that can’t be overcome through sheer force of will; a fact that my biochemical imbalance predetermines. On one hand, taking responsibility for your mental health is an important part of managing it. On the other, there’s an element of frightening imposition that comes with accepting that the very fact of your diagnosis is out of your control. I carry my depression around with me- not by choice or through lack of effort, but because its complex tangle of symptoms, neurological effects, and genetic alterations are not things I can leave behind.
Despite coming to terms with the apparent chronic nature of my depressive episodes and the fact that right now, I need antidepressants, I see this next step in mental health treatment options as Phase Two of my personal acceptance hurdle. It was tough to accept that I needed antidepressants, and now it’s tough to accept that I may benefit from another level of psychiatric treatment. I like to mull things over for a very long time, so until or if I decide to make that leap, I’m just considering it.
Did you know that immune changes are associated with Major Depressive Disorder? Let’s dive into what scientific research says about how depression affects immune system function.
Lately, I’ve been fascinated by the research on depression and immune system function. Perhaps you’re more in-the-know about this topic than I am and this doesn’t surprise you, but I was shocked to learn that not only do there appear to be measurable changes to the immune system with Major Depressive Disorder, but there are also numerous studies on it dating back decades. This isn’t a fringe area of research! Let’s take a look at how depression affects immune system function and what it means for people with depression.
The Evidence: T Cells and Depression
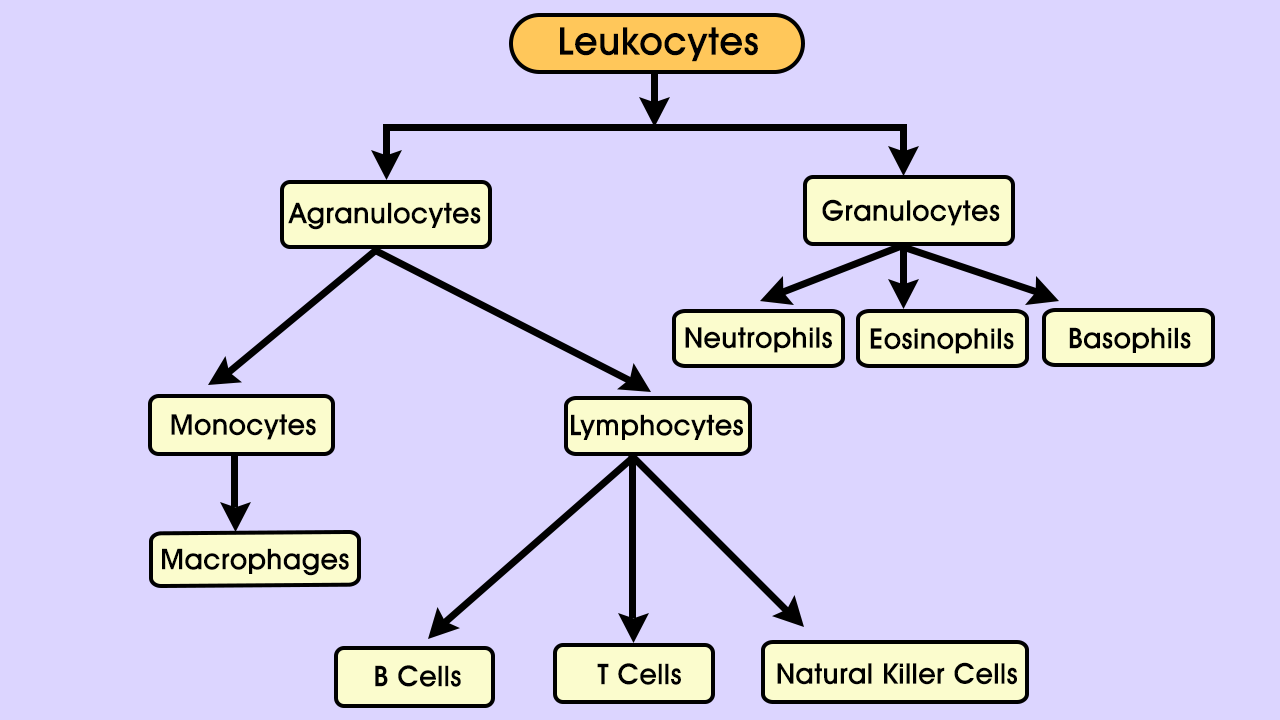
Photo frombodytomy.com
T cells are a kind of lymphocyte, which are themselves a type of leukocyte, or white blood cell. Lymphocytes are involved in what’s called adaptive immunity; they use molecules on other cells – the body’s and invading pathogens – to recognize foreign material and defend against it. Kinds of lymphocytes include T cells, B cells, and Natural Killer cells. Different types of T cells perform different roles, such as “helper” cells (Th- cells), “regulatory” cells (Treg cells), and cytotoxic cells. CD4 and CD8 (which refer to markers on the cell surface) are the two main categories of T cells. CD4 T cells are mainly helper cells, and CD8 T cells are mainly cytotoxic, meaning they mount direct attacks against invaders.
Both main types of T cells, CD4 and CD8, have other molecules attached to their surfaces. Some are receptors that grant the cell access to infections; two such receptors are known as CXCR3 and CCR6. Antidepressant-free patients with MDD have been shown to have significantly lower expression of both receptors on both types of T cells. The same study also found a significant trend in MDD towards fewer Natural Killer cells, a finding that was corroborated in another study.
Research has shown that T cells have a neuroprotective quality. T cells migrating to the brain can reduce stress, promote neurogenesis (growth and development of nervous tissue), and reduce inflammation. Study after study have found inflammation, changes in immune cell composition, receptor alterations, and gene expression changes associated with Major Depressive Disorder.
Causes and Effects of MDD Immune Changes
All of these changes are fascinating in themselves, but are they the results of depression, causes of it, or some intermediary factor?
The Sickness Behavior Hypothesis
Some researchers view depression as a maladaptive result of what’s called “sickness behavior”. Sickness behavior is a vertebrate trait that, through behaviors like somnolence, anhedonia (loss of interest or pleasure), and reduced or no eating, conserve energy that can be directed towards fighting infection. Researchers have presented evidence that both sickness behavior and depression are mediated by pro-inflammatory cytokines– proteins that act in cell signaling roles. These two observations- depression and sickness behavior share symptoms as well as mediators- led to the following hypothesis. Depression is the alternate, maladaptive pathway of molecular processes that, on the other pathway, lead to sickness behavior. Under this hypothesis, the depression pathway leads to neurodegenerative changes that make repeated episodes more likely. Adding that to other research that shows a link between sickness behavior and major depression, and a fascinating picture emerges.
Approximately 60% of people with MDD who experience a single depressive episode go on to have a second episode, and about 70% are likely to experience a third episode. Similarly, having had three episodes increases the chances to about 90% that a fourth episode will occur.
Functional Consequences
Biochemically, these changes are significant. Functionally, do they affect the people who have them? The answer may be yes. One study found a 59% increase in the risk of infection following one depressive episode. The increases weren’t linear, but the risk did go up again after the fourth episode. In addition, among college students, poor mental health is correlated with acute infectious illness.
Fortunately, treatment with antidepressants, if effective for depression, also returns T cell subsets to normal ratios. Differences in the subset ratios between those who responded to treatment and those who didn’t may help determine the chances of efficacy for a particular patient with antidepressant treatment.
I was recently flipping through a journal and came across the first poem. I remember writing it. I was sitting on a bench outside, feeling utterly defeated by depression. I had gone for a walk on a trail I’d paced a hundred times, but felt foreign on the path and in my own body. Everything heavy, I sat on a bench and looked numbly at the world around me. All the parts of being outside that I love the most- the sun, the animals, the plants- seemed wrong. The sunlight was flat, the grasses moved unnaturally, and the birds seemed oblivious to my presence- as if I had already faded away.
These days, I still walk the same trail. Sometimes it feels like a chore, and sometimes it feels just right. I listen to the meadowlarks sing and the prairie dogs yip, and moving forward is easy. One foot in front of the other, I let the motion of my legs carry me without a thought. Other days, the weight of depression demands my attention. When that happens, and I’m overwhelmed by the sense that I shouldn’t be here- I shouldn’t be anywhere- all I can do is breathe, and wait for another good day.