

Did you know that immune changes are associated with Major Depressive Disorder? Let’s dive into what scientific research says about how depression affects immune system function.
Lately, I’ve been fascinated by the research on depression and immune system function. Perhaps you’re more in-the-know about this topic than I am and this doesn’t surprise you, but I was shocked to learn that not only do there appear to be measurable changes to the immune system with Major Depressive Disorder, but there are also numerous studies on it dating back decades. This isn’t a fringe area of research! Let’s take a look at how depression affects immune system function and what it means for people with depression.
The Evidence: T Cells and Depression
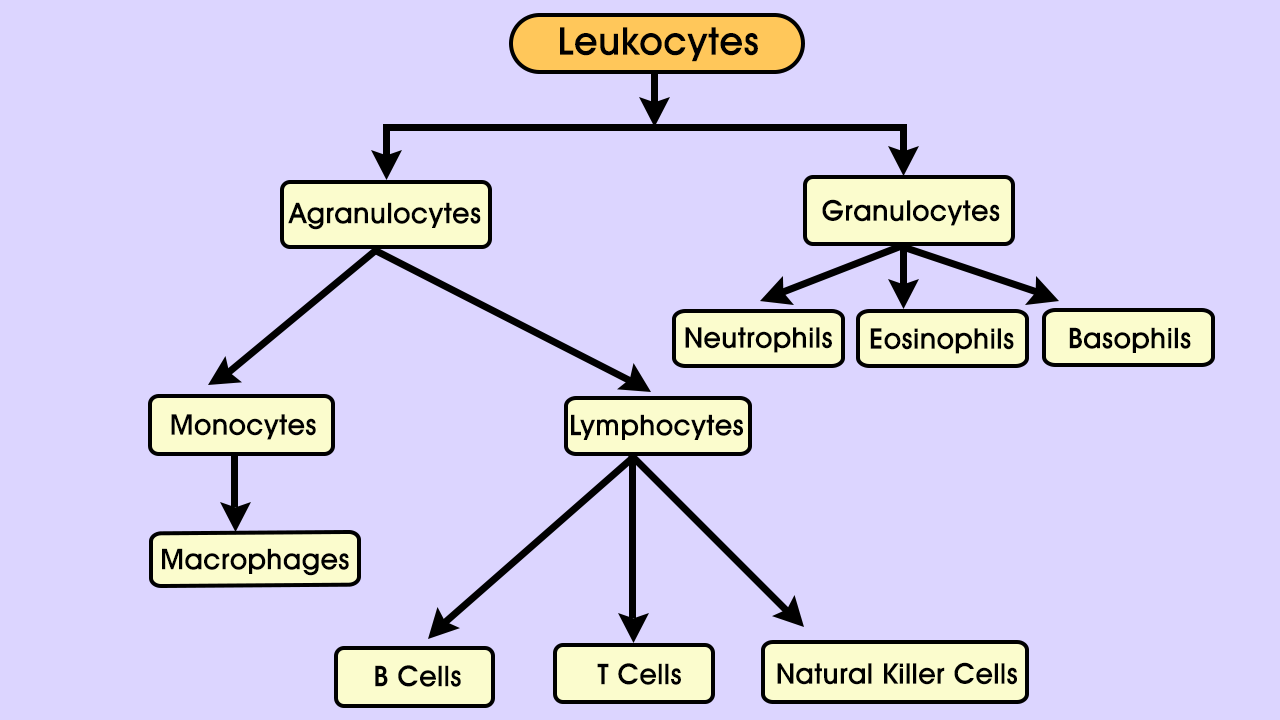
T cells are a kind of lymphocyte, which are themselves a type of leukocyte, or white blood cell. Lymphocytes are involved in what’s called adaptive immunity; they use molecules on other cells – the body’s and invading pathogens – to recognize foreign material and defend against it. Kinds of lymphocytes include T cells, B cells, and Natural Killer cells. Different types of T cells perform different roles, such as “helper” cells (Th- cells), “regulatory” cells (Treg cells), and cytotoxic cells. CD4 and CD8 (which refer to markers on the cell surface) are the two main categories of T cells. CD4 T cells are mainly helper cells, and CD8 T cells are mainly cytotoxic, meaning they mount direct attacks against invaders.
Both main types of T cells, CD4 and CD8, have other molecules attached to their surfaces. Some are receptors that grant the cell access to infections; two such receptors are known as CXCR3 and CCR6. Antidepressant-free patients with MDD have been shown to have significantly lower expression of both receptors on both types of T cells. The same study also found a significant trend in MDD towards fewer Natural Killer cells, a finding that was corroborated in another study.
Research has shown that T cells have a neuroprotective quality. T cells migrating to the brain can reduce stress, promote neurogenesis (growth and development of nervous tissue), and reduce inflammation. Study after study have found inflammation, changes in immune cell composition, receptor alterations, and gene expression changes associated with Major Depressive Disorder.
Causes and Effects of MDD Immune Changes
All of these changes are fascinating in themselves, but are they the results of depression, causes of it, or some intermediary factor?
The Sickness Behavior Hypothesis
Some researchers view depression as a maladaptive result of what’s called “sickness behavior”. Sickness behavior is a vertebrate trait that, through behaviors like somnolence, anhedonia (loss of interest or pleasure), and reduced or no eating, conserve energy that can be directed towards fighting infection. Researchers have presented evidence that both sickness behavior and depression are mediated by pro-inflammatory cytokines– proteins that act in cell signaling roles. These two observations- depression and sickness behavior share symptoms as well as mediators- led to the following hypothesis. Depression is the alternate, maladaptive pathway of molecular processes that, on the other pathway, lead to sickness behavior. Under this hypothesis, the depression pathway leads to neurodegenerative changes that make repeated episodes more likely. Adding that to other research that shows a link between sickness behavior and major depression, and a fascinating picture emerges.
Sickness behavior and major depression do look remarkably alike in their symptoms, and we do know that major depression is often a lifelong illness.
Approximately 60% of people with MDD who experience a single depressive episode go on to have a second episode, and about 70% are likely to experience a third episode. Similarly, having had three episodes increases the chances to about 90% that a fourth episode will occur.
Functional Consequences
Biochemically, these changes are significant. Functionally, do they affect the people who have them? The answer may be yes. One study found a 59% increase in the risk of infection following one depressive episode. The increases weren’t linear, but the risk did go up again after the fourth episode. In addition, among college students, poor mental health is correlated with acute infectious illness.
Fortunately, treatment with antidepressants, if effective for depression, also returns T cell subsets to normal ratios. Differences in the subset ratios between those who responded to treatment and those who didn’t may help determine the chances of efficacy for a particular patient with antidepressant treatment.


