May is Mental Health Awareness Month! One lesser-tackled mental health topic (in my opinion) is that of periods and mental health.
Invalidation: Public and Self
We often see in media the idea that a woman on her period is “crazy”- invalidating language that means it’s ok for others to ignore her feelings. I think it’s important to recognize that the hormonal changes we experience don’t suddenly make us different people. I, for one, become rather cranky, but not because I’ve developed a new set of preferences and opinions; I just have a lower tolerance for irritation. A much, much lower tolerance. Things that at any other time would simply make me shake my head suddenly either make me briefly, intensely angry or likely to burst into tears.
I find myself downplaying the effects of my period on my mental health all the time. I think it stems from its temporary nature. I know that it won’t last long, so it seems silly to let it take up much space on my list of mental difficulties. When I’m seeing red because somebody put a spoonful of cooked rice in the dishwasher and ran it, I invalidate myself. I tell myself that how I feel doesn’t matter because it’s caused by temporary hormones and my reaction is disproportionately intense. And it is temporary and more intense than is warranted. But the reality is, it’s extremely uncomfortable to experience month after month. Each small instance of unreasonable mood swinging adds up to something with tangible impact.
But it’s ~Natural~
Having a healthy menstrual cycle is a positive thing! If women for millennia have been dealing with theirs, why should I let mine be a roadblock for me? I’m sure women millennia ago thought it sucked just as much as we do, if not more. Modern methods of dealing with it hygienically and the availability of painkillers probably makes menstruating a good deal more comfortable for us. (Of course, there’s a conversation to be had about poverty’s restriction of women’s access to these modern resources. Not everyone enjoys the comforts of disposable period products. Here’s a good resource for learning about period poverty.)
There are definitely positive ways of talking about periods; their position in the menstrual cycle plays a vital role in fertility and reproduction, after all. That doesn’t eliminate the damage that periods can do to our mental health, however. We can recognize the beauty of a natural, cyclical process while also shaking our collective fists at Mother Nature.
Photo by Natracare on Unsplash
PMS and Depression
As many as 3 in 4 women experience PMS. Symptoms include mood swings, irritability, crying spells, social withdrawal, and a host of uncomfortable physical symptoms. That alone is more than enough to be impactful when it comes to a person’s periods and mental health. And what about people who have a mental health diagnosis in addition to PMS? According to the Office on Women’s Health, “Many women seeking treatment for PMS have depression or anxiety. Symptoms of these mental health conditions are similar to symptoms of PMS and may get worse before or during your period.”
Personally, I can say with certainty that when I’m really struggling with my depression, my suicidal thoughts and the urges to self harm are worst leading up to and during my period. In fact, my period started a few days into my hospitalization in 2019 – a connection that I only made later on. The effects of the hormonal changes may be temporary, but my period is a setback to my mental health on a regular basis. And with an extremely serious thing like suicidal ideation, any factor that worsens it is nothing to be dismissed. Sometimes, even when things are getting better, I have sneaky, destructive thoughts because of hormonal fluctuations.
In those cases, it is helpful to remember that my period is to blame and that it will pass. I have to strike a balance, though. It’s easy for me to bully myself into feeling bad about slip ups and setbacks because “it’s just my period.” Hormones are powerful and their effects are very real, no matter how temporary.
Managing Periods and Mental Health
There are many ways to manage PMS for a better relationship between your periods and mental health. Many people find that lifestyle changes through diet, exercise, and healthy sleep are enough to improve their PMS, but your doctor might suggest other options as well. Hormonal contraceptives can help even out the dramatic peaks and valleys of hormone changes. For some people, PMS rises to the level of PMDD, or premenstrual dysphoric disorder. This can be treated through a variety of interventions.
It’s unfortunate that conversations about the mental health effects of the menstrual cycle are reserved only for certain private settings and are kept to a quiet minimum. Periods are a fact of life for many people. We should be able to discuss them openly as a legitimate factor affecting mental health. A survey of 1,500 women found that 58% have been embarrassed about their period at one point or another. 62% of respondents were uncomfortable even using the word “period.” Thankfully, there are many initiatives fighting stigma and working to provide resources to women and girls around the world, and we can keep the conversation going.
How does your period impact your mental health? Have you experienced period shame?
Social, Psychological, and Diagnostic Aspects of Depression in Men
Four times more men die by suicide than women, and yet half as many men are diagnosed with depression as are women (1). In researching this topic, I was encouraged by the shift our society is making towards understanding depression in men and the factors that push them to such lengths. However, there is clearly still a long way to go. A book I skimmed early on in my search, aptly titled Men and Depression, by Sam Cochrin and Frederic Rabinowitz, mentions in the introduction that “A book that examines distress and depression in men may be seen by some as politically provocative.” In 2000, when that book was published, many researchers and clinicians were working to move public perception of mental disorders in men inch by inch. They recognized that the disparity between the number of men diagnosed with depression and the number of men who kill themselves indicates a hidden population of men who battle their depression in secret. 21 years later, the number of articles under a “depression in men” search in Google Scholar numbers over 3.5 million.
As a woman who suffers from depression, I feel relatively safe in disclosing my diagnosis. People are generally sympathetic and understanding when I discuss my symptoms. But how do men feel about the way their depression is received? A man I know has been dealing with depression for a long time, so I asked him exactly that question. Thankfully, he told me that his social circles have been largely supportive, which I think is an encouraging sign for our culture’s direction. But what factors make the rates of suicide between men and women so different? If we’ve come from “politically provocative” to millions of research articles in two decades, why are many men still suffering in silence? I want to dig into this issue to understand the historical trends, what sometimes makes depression in men different, and what we can do to keep the conversation going.
Historical Epidemiology of Suicide
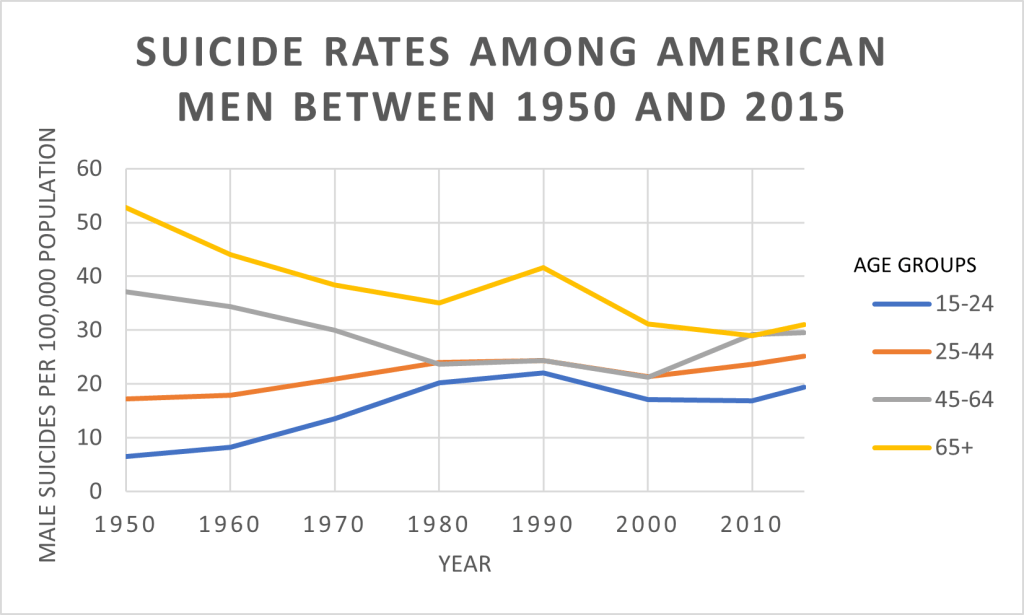
In a really deep dive, we could go way back to Hippocrates and Galen to explore the perceived gender divide on mental disorders, which would be interesting. But in this context, we’ll stick to the 20th and 21st centuries. Let’s take a look at this set of data from the CDC’s Data Finder (12). It’s compiled mostly by decade between 1950 and 2015. This graph of the data, which I made with my rusty skills in Excel, illustrates the suicide trends by rate among men in various age groups.
Although the rate of suicide among all ages has remained relatively stable, trends within age groups are concerning. Suicides among 15-24 year-olds have increased dramatically, as have those among 25-44 year-olds. Despite a somewhat steady decline in the suicide rate of men aged 65 and older, they remain the group with the highest rate. By 2019, the rate of suicide in men had increased from 21.1 deaths per 100,000 to 23 deaths per 100,000 (13). For every 100,000 men, 23 deaths doesn’t immediately sound shocking. But to illustrate the numbers in a different way, consider that in 2019, a horrifying total of 37,256 men killed themselves in the U.S.
It introduces another layer of complexity to compare the data on men to the data on women. The suicide rate among women of all ages has increased since the 50’s more than it has among men, but it still sits markedly lower. In 2019, the overall suicide rate among women was 6.2 deaths per 100,000 people (13). Compared to 37,256 male suicides, the country saw 10,255 female suicides. Both of those numbers are unimaginable to me, but it’s worth investigating; why is the rate for men so much higher than it is for women?
Photo by Mykyta Martynenko on Unsplash
Diagnostic Factors
The wildly higher rate of suicides among men than in women, combined with the average 2:1 ratio of depression diagnoses in women versus men, convincingly suggests that depression in men is going undiagnosed. An increasingly accepted hypothesis regarding this conclusion is that depression in men and women can be experienced in different ways (10). The current diagnostic tools don’t capture all of the symptoms of depression that men commonly face. The gender differences in symptomatology have led some to argue for the recognition of separate depression diagnoses for men and women. Magovcevic and Addis conceptualized the differences as constituting typical depression plus a subtype, masculine depression (6). Subsequent research shows that some men who don’t fully fit the diagnostic criteria on traditional depression questionnaires may be diagnosed when masculine depression symptoms are considered.
Masculine Depression Symptoms
“Masculine depression” (also called male depression and a variety of other terms), is characterized by more symptoms of anger, aggression, risk taking, and substance abuse than tend to occur in women. These symptoms are examples of “externalizing features.” They serve to express a person’s emotions in an outward, active way. “Internalizing features” of depression are identified by retreating into one’s self, such as by ruminating, engaging in negative self-talk, and isolating from others.
New Self-Report Scales
To investigate the efficacy of adjusted self-report scales at identifying depression in men, researchers created the Gender Inclusive Depression Scale (GIDS) using two other male depression scales validated with small cohorts. When symptoms of masculine depression – the externalizing features – are included in a traditional diagnostic survey, the rates of depression diagnoses among men and women are not significantly different (7). In other words, the gender differences disappear. Another scale, the Male Depression Risk Scale (8), measures emotion suppression, drug use, alcohol use, anger and aggression, somatic symptoms, and risk-taking. The sensitivity of the MDRS is similar to that of the PHQ-9 in recent suicide attempt identification (9).
Why is Depression in Men Sometimes Different?
To be clear, it’s a continuum; many men are diagnosed with depression using traditional questionnaires. But for the ones who aren’t, the answer is probably based in gender norms. Men who have depression and who identify with traditional ideals of masculinity are more likely to experience masculine depression symptoms (4). In a society that has traditionally viewed men who express sadness as “weak” or “feminine,” it makes sense that sometimes, depression in men is displayed as anger or in attempts to cope with it through substances. Sadly, it’s more socially acceptable for men to express anger than sadness, self-doubt, or anxiety.
Photo by Andre Hunter on Unsplash
Why is the Suicide Rate Among Men so Much Higher?
If newer diagnostic scales indicate that the rates of depression in men and women are actually more alike than previously thought, what is going on with the suicide rates? Why would men die by suicide four times more often than women? It’s hard to know how many suicides could have been prevented by mental health intervention, but it’s logical to think that men who aren’t seeking counseling or who are dismissed without a diagnosis would be more likely to turn to suicide as the answer. Additionally, we know that although men complete suicide more often than women, women attempt it more often (11). Men tend to use more lethal methods, and for some men, the act of suicide represents an affirmation of strength and independence (2). It is crucial that we improve identification and treatment of depression in men (5).
A Note on “Masculine” and “Feminine”
With all of this discussion about a “masculine” depression facet, I have a small fear that readers of this post will leave feeling as though their diagnosis of depression must have been of the feminine kind. It’s not. It’s just depression – men, women, nonbinary people – it doesn’t impose judgment on your identity, it simply is. Just as men may experience more anger and impulsivity as part of their depression, women may be more likely to suffer body image issues and self-harm behaviors. But it’s a bell curve; just because men are more likely than women to exhibit anger as a sign of depression doesn’t mean that women can’t as well. Statistically, neither gender is more closely associated than the other is with the typical symptoms (8). The only gendered difference exists in the subset of “masculine” symptoms. The core set of symptoms that are covered in typical scales like the PHQ-9 remain the main diagnostic components of what we know depression to be. Expanding the criteria by creating a subset of symptoms more associated with men is just a way of widening the net in order to keep people from falling through the cracks.
For more reading on how men can view depression, suicide, and masculinity, check out this article. The author provides evidence for a variety of views that men hold about how mental health and suicide relate to masculinity.
Identifying Depression in Men Going Forward
For a long time, our definition of depression was too narrow. The research on gender differences in depression, which I have only barely scratched the surface of, is vast and still growing. Although the standard depression questionnaires remain focused on internalizing features to the exclusion of the externalizing ones, authorities on the matter have acknowledged the issue in other ways. The American Psychiatric Association has a webpage from 2005 that describes the early research and what to watch out for in men who may have depression. They now have a number of web pages, magazine articles, fact sheets, and books about men and depression. Someday, I hope that standard depression questionnaires will include measures for symptoms that men exhibit, but until then, we can continue to reduce stigma and spread the word about how depression in men can manifest.
Photo by Marco Bianchetti on Unsplash
You can pass online resources on to the men you know. You can talk about it with your doctor. You can listen to your friends, fathers, brothers, and sons. Assure them that having feelings doesn’t make them less of a man, it just makes them human.
Resources
National Suicide Prevention Lifeline: 1-800-273-TALK (1-800-273-8255)
Keohane, Aisling, and Noel Richardson. “Negotiating Gender Norms to Support Men in Psychological Distress.” American Journal of Men’s Health, October 11, 2017. https://pubmed.ncbi.nlm.nih.gov/29019282/.
Magovcevic, Mariola, and Michael Addis. “The Masculine Depression Scale: Development and Psychometric Evaluation.” APA PsycNet, 2008. https://psycnet.apa.org/record/2008-09203-001.
Martin, Lisa, A, Harold Neighbors W, and Derek Griffith M. “The Experience of Symptoms of Depression in Men vs Women: Analysis of the National Comorbidity Survey Replication.” JAMA Psychiatry, October 2013. https://jamanetwork.com/journals/jamapsychiatry/fullarticle/1733742.
Rice, Simon, M, and Anne-Maria Moller-Leimkuhler. “Development and Preliminary Validation of the Male Depression Risk Scale: Furthering the Assessment of Depression in Men” 151, no. 3 (December 2013): 950–58.
Rice, Simon, M, John Ogrodniczuk S, David Kealy, and Zac Seidler E. “Validity of the Male Depression Risk Scale in a Representative Canadian Sample: Sensitivity and Specificity in Identifying Men with Recent Suicide Attempt.” Journal of Mental Health, November 2017, 132–40.
Rutz, Wolfgang, Jan Walinder, and Lars Von Knorring. “Prevention of Depression and Suicide by Education and Medication: Impact on Male Suicidality.” International Journal of Psychiatry in Clinical Practice, January 8, 1997. https://www.tandfonline.com/doi/abs/10.3109/13651509709069204.
Did you know that immune changes are associated with Major Depressive Disorder? Let’s dive into what scientific research says about how depression affects immune system function.
Lately, I’ve been fascinated by the research on depression and immune system function. Perhaps you’re more in-the-know about this topic than I am and this doesn’t surprise you, but I was shocked to learn that not only do there appear to be measurable changes to the immune system with Major Depressive Disorder, but there are also numerous studies on it dating back decades. This isn’t a fringe area of research! Let’s take a look at how depression affects immune system function and what it means for people with depression.
The Evidence: T Cells and Depression
Photo frombodytomy.com
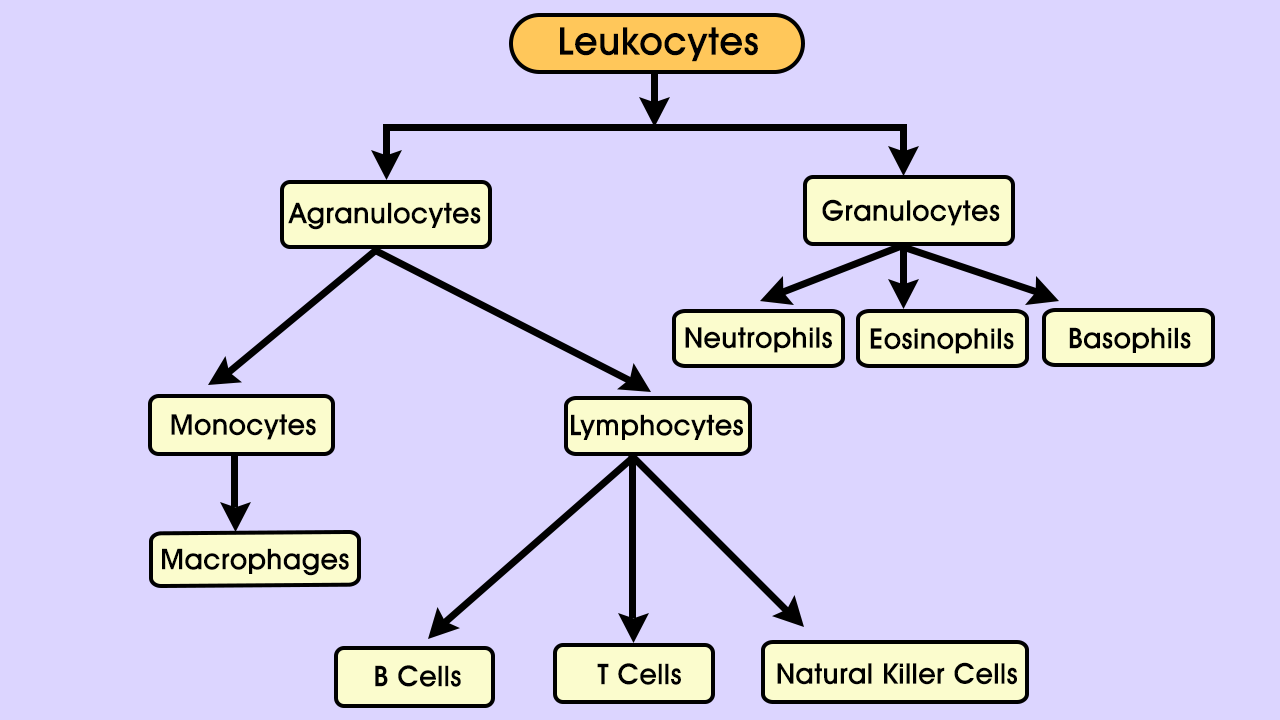
T cells are a kind of lymphocyte, which are themselves a type of leukocyte, or white blood cell. Lymphocytes are involved in what’s called adaptive immunity; they use molecules on other cells – the body’s and invading pathogens – to recognize foreign material and defend against it. Kinds of lymphocytes include T cells, B cells, and Natural Killer cells. Different types of T cells perform different roles, such as “helper” cells (Th- cells), “regulatory” cells (Treg cells), and cytotoxic cells. CD4 and CD8 (which refer to markers on the cell surface) are the two main categories of T cells. CD4 T cells are mainly helper cells, and CD8 T cells are mainly cytotoxic, meaning they mount direct attacks against invaders.
Both main types of T cells, CD4 and CD8, have other molecules attached to their surfaces. Some are receptors that grant the cell access to infections; two such receptors are known as CXCR3 and CCR6. Antidepressant-free patients with MDD have been shown to have significantly lower expression of both receptors on both types of T cells. The same study also found a significant trend in MDD towards fewer Natural Killer cells, a finding that was corroborated in another study.
Research has shown that T cells have a neuroprotective quality. T cells migrating to the brain can reduce stress, promote neurogenesis (growth and development of nervous tissue), and reduce inflammation. Study after study have found inflammation, changes in immune cell composition, receptor alterations, and gene expression changes associated with Major Depressive Disorder.
Causes and Effects of MDD Immune Changes
All of these changes are fascinating in themselves, but are they the results of depression, causes of it, or some intermediary factor?
The Sickness Behavior Hypothesis
Some researchers view depression as a maladaptive result of what’s called “sickness behavior”. Sickness behavior is a vertebrate trait that, through behaviors like somnolence, anhedonia (loss of interest or pleasure), and reduced or no eating, conserve energy that can be directed towards fighting infection. Researchers have presented evidence that both sickness behavior and depression are mediated by pro-inflammatory cytokines– proteins that act in cell signaling roles. These two observations- depression and sickness behavior share symptoms as well as mediators- led to the following hypothesis. Depression is the alternate, maladaptive pathway of molecular processes that, on the other pathway, lead to sickness behavior. Under this hypothesis, the depression pathway leads to neurodegenerative changes that make repeated episodes more likely. Adding that to other research that shows a link between sickness behavior and major depression, and a fascinating picture emerges.
Approximately 60% of people with MDD who experience a single depressive episode go on to have a second episode, and about 70% are likely to experience a third episode. Similarly, having had three episodes increases the chances to about 90% that a fourth episode will occur.
Functional Consequences
Biochemically, these changes are significant. Functionally, do they affect the people who have them? The answer may be yes. One study found a 59% increase in the risk of infection following one depressive episode. The increases weren’t linear, but the risk did go up again after the fourth episode. In addition, among college students, poor mental health is correlated with acute infectious illness.
Fortunately, treatment with antidepressants, if effective for depression, also returns T cell subsets to normal ratios. Differences in the subset ratios between those who responded to treatment and those who didn’t may help determine the chances of efficacy for a particular patient with antidepressant treatment.
We all have those sneaky thoughts that come unbidden when we make a mistake or are faced with a change. I don’t know a single person who hasn’t mentally beat themselves up over a perceived shortcoming. Often, it isn’t deserved. But when your automatic thoughts are that you deserve those thoughts, what do you do?
“Automaticity is granted if the perceiver lacks awareness of the process, does it with efficiency (i.e., with minimal use of cognitive resources), has no intention to do it, or cannot control it.”
Based on this definition, automatic thoughts include those about others, such as deeply held prejudices. It also includes the intrusive thoughts that characterize Obsessive Compulsive Disorder, but I’ll be focusing more on those automatic thoughts that don’t necessarily play a direct role in psychopathology. For example, self-referential thoughts like, “I’m going to fail this exam. I always fail.” Those are the types of thoughts I’m talking about here.
Negative Automatic Thoughts
The most well-known measure in this area is the Automatic Thoughts Questionnaire (ATQ), a 30-item instrument developed in 1980. The ATQ contains statements like “I am a failure,” and asks participants to rate each statement on a scale representing the frequency with which they experience that thought. It’s a cross-validated questionnaire that’s been shown in several studies to correlate with depression and separate depressed from non-depressed individuals.
When presented with a distressing stimulus, previously depressed participants and people who have never been depressed experienced stronger belief in negative automatic thoughts. The researchers propose that cognitive reactivity is related to relapse and recurrence of depression.
Cognitive reactivity refers to the triggering of negative thought patterns by small declines in mood. The ability to resist slipping into negative cognitions seems to have a protective effect; inpatient surveys taken at two time points show that decreases in negative automatic thoughts are strongly correlated with reduced suicidal ideation.
Positive Automatic Thoughts
The relationship between negative automatic thoughts and depression and anxiety is well documented. We can infer that the lackof negative automatic thoughts has beneficial effects on mental health, but this still isn’t quite the same as the presence of positive automatic thoughts. However, research does support the assumption that positive thinking is related to positive mood. A variation of the ATQ was developed to measure positive automatic thoughts. It’s called the ATQ-P, and higher scores on it are strongly associated with lower levels of depression. A healthy balance of positive and negative thoughts appears to be weighted toward more positive than negative- a ratio of 0.62 to 0.38, to be exact (according to one study).
Where Exactly Do Automatic Thoughts Come From?
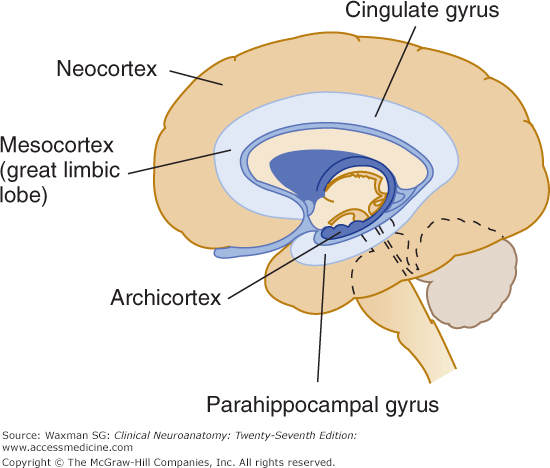
Parahippocampal gyrus
One area of the brain that is linked to automatic thoughts is the parahippocampal gyrus, a part of the limbic system.
“The voxel-based morphometry results showed that the GMV of the right parahippocampal gyrus and fusiform gyrus and the WMV of the right superior temporal pole increased with the severity of depression.”
Let’s break that down. A voxel is a value assigned to a three-dimensional grid. Think “pixel” but with volume. Voxel-based morphometry is a technique for assessing differences in brain volume. Brain scans are registered to a standard, voxel-based template, then each voxel is “smoothed” by averaging it with the values of the surrounding voxels. Finally, the image volume of each scan is compared to the other scans’ volumes and the differences between voxels are evaluated statistically. Basically, it’s a way to quickly compare lots of structural brain scans using computers.
The study found that increases in the volume of grey and white matter in certain regions of the limbic system are associated with increasing severity of depression, as measured with the ATQ. So, negative automatic thoughts are associated with depression, and depression is associated with higher volume in the emotional center of the brain. That doesn’t necessarily mean that negative automatic thoughts are directly related to grey and white matter volume. Or does it?
Statistical tests showed that the combination of automatic thoughts and grey matter volume in the parahippocampal gyrus predicted depression measured by the ATQ and the Self-Rating Depression Scale. The automatic thoughts mediate the relationship between volume and depression. They also seem to mediate the relationship between neuroticism and depression.
Medial Prefrontal Cortex
The medial prefrontal cortex is not part of the limbic system. It’s located at the very front of your brain and is associated with the processing of social information. Hyperactivity in this region has been linked to neuroticism and self-generated thought. The tendency to worry and impose self-generated beliefs onto a reality that doesn’t match those beliefs sounds a lot like the automatic thoughts in the studies above. But it’s not all bad; the same hyperactivity and self-generated thoughts are also associated with creativity.
Combatting Negative Automatic Thoughts
Hopefully, you haven’t read all of that and decided that the next time someone tells you to be more positive you’ll just say “the grey matter in my parahippocampal gyrus says, ‘No can do.'”
Photo by @linkedinsalesnavigator on Unsplash
Cognitive behavioral therapy has been shown to result in reductions of automatic thoughts and dysfunctional attitudes associated with non-clinical depression. CBT makes use of behavioral experiments and automatic thought records. People perceive behavioral experiments to be more powerful than combatting automatic thoughts with logic alone, which could be because behavioral experiments function through emotion-based cognitive systems. Mindfulness has also been shown to reduce automatic thoughts, and it’s associated with increased life satisfaction.
There are plenty of reasons to believe that we have the power to effect change in our own brains.
What helps you recognize negative automatic thoughts, and how do you practice self-compassion?
I’m hoping to make this the first post in a series called “Science Saturdays” (now taking suggestions for a more creative name) where I dive into the research at the intersection of mental health and (fill in the blank). I dipped my toes into these waters with previous posts like “Pets and Mental Health“, “Can You ‘Grow Out Of’ Childhood OCD?“, and “What’s the Deal with MTHFR and Psychiatric Conditions?” My intention is to take an objective look at recent research, let it percolate through my noggin while I sift through the dozens of tabs I’ve amassed in Google Scholar, then report back with what I think are some important takeaways.
Here in the northern hemisphere, we’re perched on the cusp of spring, and boy, am I ready to get outside. I live in Colorado, and hiking is one of, if not the most, enjoyable ways I spend my time in the warmer months. I’ve been gazing longingly at the mountains, perusing dog backpacks (that’s backpacks for dogs to wear) on Amazon, and figuratively dusting off my trail map app in anticipation. It could just be that I’m particularly drawn to being outside because of my personality and upbringing, but I’ve recently come across some buzz surrounding the positive effects that nature has on our emotional and physical health. So, I figured, what better way to become even more entrenched in spring fever than to spend a few hours reading about the outdoors?
Nature and Physical Health Studies
Nearly every article I’ve read so far has referenced a study published in 1984 by RS Ulrich. The study looked at a group of 46 hospital patients, all of whom had their gallbladders removed and were monitored postoperatively. 23 patients stayed in rooms with views of trees, while the other 23 had views of a brick wall. The now classic study found that the patients who had views of trees recovered faster and required less pain medication than the other group of patients.
Increasingly, researchers are investigating the relationship between biodiversity in green spaces and psychological benefits. Several nature and mental health studies have found significant associations between higher plant and bird diversity and positive mental effects. A 2007 study by Fuller et al. found a positive correlation between plant species richness and participants’ sense of identity and ability to reflect. The 312 participants were fairly accurate at assessing plant species richness, which muddies causality. The question then becomes: are the benefits derived from species richness or perceived species richness?
Here’s another study to elaborate on that distinction. Researchers here found that psychological benefits of nature exposure were correlated not with biodiversity, but with participants’ perception of biodiversity only. In this study, participants were apparently not at all good at estimating species richness, and it affected their experience of being outside, regardless of how many species were actually present.
Frequency and Duration of Nature Exposure
So it seems that the more varied and species-rich the environment, the better. But is glancing out a window now and then the same as going for a walk outside, psychologically? I’d say no, but that doesn’t mean that short exposures to nature don’t benefit us. After all, just a 40-second break to look at a green, plant-filled roof has been shown to improve attention and performance on cognitive tasks, as compared to a break of the same length with views of concrete roofs.
In a sample of over 1500 Australian respondents, longer duration of nature excursions is associated with decreased prevalence of depression and high blood pressure. More frequent visits to public green spaces are associated with a greater sense of social cohesion, which I imagine contributes positively to mental health in general.
Criticisms of Nature and Mental Health Research
Few studies on the topic of nature and mental health take an epidemiological approach, leading some to point out that we have very little data on long-term, population-level health effects of nature exposure. Criticisms of some studies also include sample size, lack of adequate controls, and statistical rigor. However, the number of studies that demonstrate a correlation between nature and mental health benefit vastly outweigh the number of studies that show no relationship. While this does not negate the weaknesses mentioned previously, it does seem to suggest that there is validity to the idea that nature is emotionally beneficial.
The Daffodils are Blooming
All the signs that winter is ending are here; the daffodils are blooming, more birds are singing, the neighbors are cleaning out their garage, and before spring really gets underway, Colorado is scheduled to get one or two more last-minute dumps of snow.
Speaking of, now that I’ve gotten myself extra excited to get outside and let my brain soak in the wonderful sights, sounds, and smells of spring, it’s time to prepare myself for tonight’s snowstorm.
When I was 10, I felt compelled to tell my parents “I love you” every time they left the house. Going to the grocery store? I love you. Going to work? I love you. Going to the mailbox? I love you. The fear that something catastrophic will happen to family members is a common manifestation of childhood and adolescent OCD. I thought that if I failed to carry out this ritual, my parents wouldn’t know that I loved them if or when something terrible occurred.
I was also preoccupied with germs; my hands were cracked and bleeding from excessive washing, and I worried constantly about contamination. I always walked a specific pattern on the rug in the hallway, and I carefully watched the family dog to be sure I’d notice when he winked at me–so that I could wink back. I couldn’t tell you why I had to wink at the dog, I just had to.
I knew that these behaviors were irrational, and yet the anxiety it caused me to resist the compulsions seemed unbearable. I was afraid to go to sleep because I worried I might sleepwalk and harm my family in the middle of the night. Nearly every evening, I would tearfully confess my intrusive thoughts to my mother, convinced that she would be afraid of me for thinking such awful things. OCD commanded almost every aspect of my life.
Did I Grow Out Of It?
My parents tried to get me into therapy, but I was shy and ashamed, and simply refused to participate. So, I started taking an SSRI, slowly titrating up to the maximum dose. And incredibly, it worked. Suddenly, I was free from the torturous anxiety and embarrassing compulsions. I could be a kid again. Two years on, I slowly came off my medication. We waited, on edge, for symptoms to return, but they never did. I’ve often wondered why I never relapsed. It seemed impossible that something that had plagued me for so long had just vanished.
Thanks, PubMed
I wanted to know if other people had experiences similar to mine, so I headed over to trusty ol’ PubMed. I found several articles that explore the topic of OCD remission. Some have woefully small sample sizes and others are barely longitudinal, but there does seem to be a higher rate of OCD remission in the pediatric population than the adult population. The factors that influence this aren’t very well understood; some studies show that an earlier onset of symptoms predicts better outcomes, while others associate earlier onset with chronic, adult OCD. Don’t you just love conflicting results? I do, however, think these results can be reconciled.
Maybe It’s About Treatment, Not Age
A study published in 2014 followed up with children and adults with OCD over a three-year period. Children achieved remission more quickly than adults who had juvenile-onset of symptoms, but the age of onset did not affect the likelihood of remission. Instead, the authors show that the less time passes between the onset of symptoms and receiving treatment, the better the outcome.
This fits with the statistics on OCD treatment. In a different study by the same authors, children went an average of 1.5 years before receiving treatment, whereas adults reported a wide range of latency periods. On average, they went 14.5 years before receiving treatment, although the standard deviation was close to 12 years. Clearly, some adults suffer in silence for decades before getting treatment.
It’s plausible, then, that children who receive treatment soon after developing symptoms see remission more often, but children who endure a longer period of uninterrupted symptoms are more likely to have chronic OCD into adulthood.
The Takeaway
Multiple studies emphasized the importance of early recognition and treatment of childhood-onset OCD. Overall, I was encouraged by what I found during my deep dive into the literature. The sources I found all seemed to agree; long-term persistence of childhood-onset OCD is less common than it is for adult-onset OCD.
After all this, I’m still not sure whether I grew out of OCD. It’s difficult to determine whether anybody grows out of it without treatment because study samples come largely from inpatient and outpatient treatment centers. I will say that I occasionally get a sticky thought that reeks of OCD, but I set it aside fairly easily.
In a completely anecdotal way, this seems to me like the pathways that I was stuck in as a child had a chance to be rewired while I was on medication. Now, my brain can cope with intrusive thoughts pretty much like anybody else’s. If I had known that the chances were pretty good that I wouldn’t suffer from OCD forever, it might have been a little easier to cope as a child.
Treatment with ERP and medication offers adults and children relief from their OCD symptoms. So, if you have a kid with OCD, know that remission is possible. And for all the adults with OCD, know that there is hope, and you are not alone. Adults absolutely achieve remission as well. A 40-year follow-up study found that of 251 participants, improvement was observed in 83%. Those are pretty good odds!