When some questions about my diagnosis arose a couple months ago, I realized that my medications made it difficult to determine which symptoms were side effects and which were stemming from me. I’ve wanted to get off my meds for a long time, partly because I have an unhealthy tendency to blame myself for my illness and expect myself to fix it through willpower. But that’s a whole separate issue. Don’t do as I do in that regard.
I decided to get off Emsam first, as I suspected that was the main culprit when it came to the occasional hallucinations and sudden mood shifts I was experiencing. Decreasing my dose was difficult, but when I stopped taking it completely, I felt better. Not by a lot, but it was noticeable.
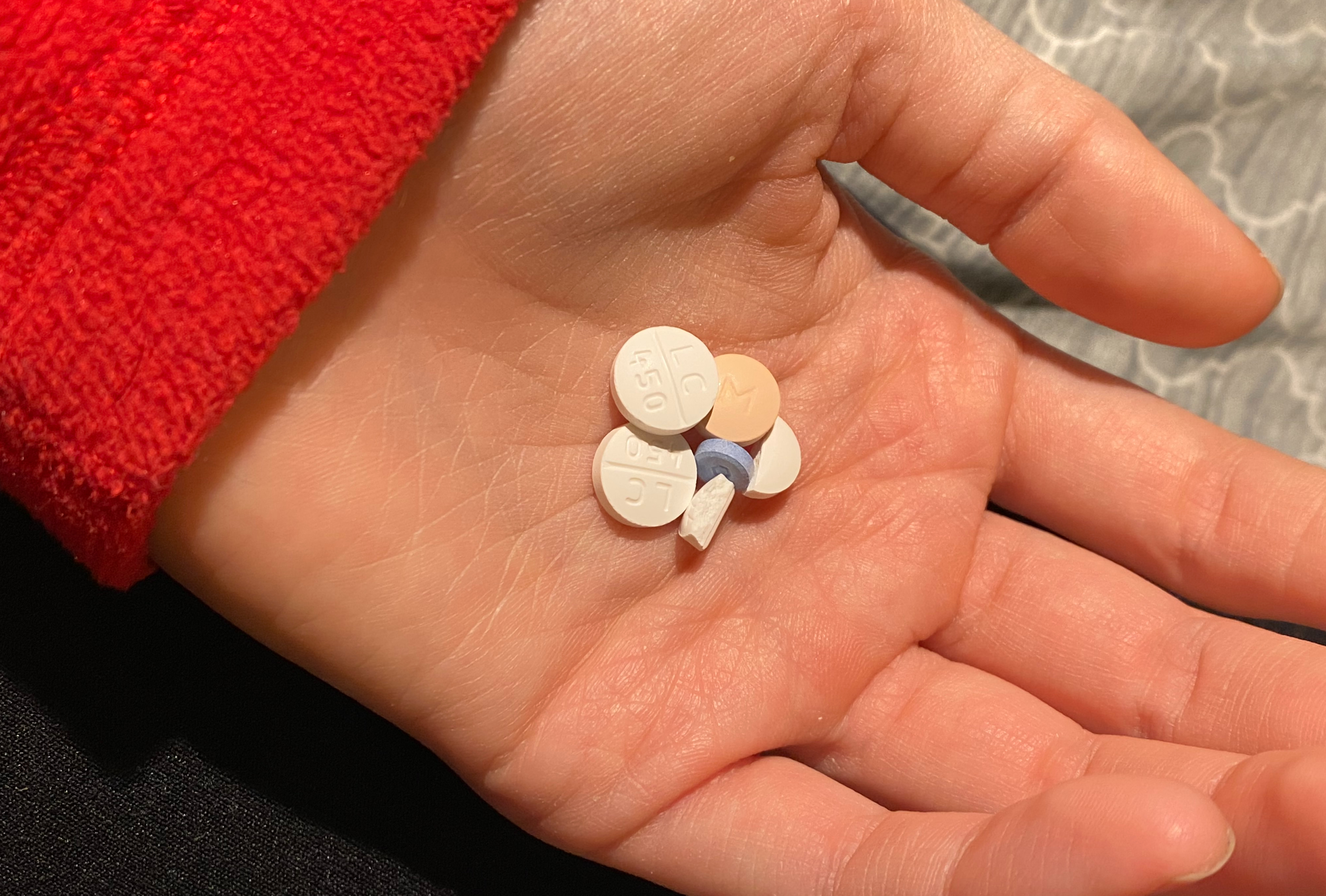
The next step was to decrease my lithium dose. That process has progressed in the reverse of how Emsam went. Lowering it was mostly fine until I got to 300 mg. I started to feel worse, but I hoped that if I stayed at that dose for a while, my mood would even out. I started napping again. If I have nothing scheduled in the afternoon, I spend it sleeping. Walking Stella was one of the only activities I was enjoying before I started changing my meds, and now I don’t even want to do that. I still take her on at least one long walk a day because she needs it, but I find myself getting irritated and impatient the farther we get from home. Sometimes we go to the dog park so I can stand in one place and throw a ball for ten minutes before we leave. It’s a good thing she likes fetch.

I stopped taking lithium over a month ago, and I’m still on the fence about it. I’ve definitely crossed into not-okay territory, but I’m stubbornly refusing to reverse my plan. Part of me thinks this is a bad idea and I should go back on lithium, but part of me wants so badly for it to work out that I’m willing to give it more time.
My determination to get off my medication, even though it has a slightly positive influence, seems confusing on the surface, and I struggle to articulate my reasoning for it. I always think that I’m not doing enough to help myself, and I have a long history of feeling ashamed of my reliance on medication. I think the most succinct way I can describe it is that I’d rather believe I’m failing at doing something possible than accept that it’s impossible. Truly accepting that I need medication in order to function would require me to admit that I don’t have full control over myself, and that’s a frustrating and scary thought for a perfectionist.
I’ve mentioned this in previous posts, but to be clear: I don’t feel this way about anyone else. It’s a bizarre thought distortion that makes me feel as though everyone else is perfectly justified in taking medication, but I am not. The more depressed I get, the harder it is to see the irrationality of that.
I’m trying to push myself to do things and go places because I want to support my mental health as much as possible while I make these medication changes. It’s hard, though. The holiday season is upon us, and the twinkling lights and pine-bough wreaths on nearby homes are making me sad. I automatically think about all of our holiday decorations burning up in the fire five days after Christmas last year. I felt like I was moving on during the summer, but the cold weather has caused a resurgence of painful memories. It’s probably not the best time for me to be messing with my brain chemistry, but here we are.
I’m just so frustrated with medications. The possibility that I have bipolar disorder offers a nice, neat explanation for why I’ve had such sporadic and limited success with antidepressants. Getting off everything so that I can tell where my baseline is (and whether I eventually cycle back into hypomania without the influence of mood stabilizers) might make a difference in my plan going forward. The diagnosis is arguably not as important as figuring out what helps me, but since I tend to spiral into believing I’m not actually ill but rather just low in the willpower department, having a name for what I’m experiencing would be helpful. I’m just not sure if it’s worth the difficulty of achieving confidence in one diagnosis over the other, and it’s obviously not going great so far.
In fact, my mood has sunk so low that I agreed to retry ketamine – but in a different format this time. My psychiatrist prescribed ketamine troches, which dissolve under your tongue. This formulation of ketamine can be taken at home, which would be new for me. I’m nervous about it – for one thing, it’s much less controlled, in the sense that an IV ketamine infusion can be stopped suddenly; once I take the troche, I’ll just have to wait out the whole dose. I started to really dislike the feeling of ketamine toward the end of my time getting infusions, and although I don’t think troches will feel as intense, the uncertainty is making me anxious.
I am, however, passively suicidal and having trouble keeping up with self-care. I frequently sleep in my clothes and re-wear them the next day, and my hair keeps developing hidden matted sections because I can’t bring myself to brush it. So, perhaps something like a short burst of at-home ketamine would help me get myself into a better routine.
My depression brain is yelling about how I got myself into this mess by stopping my meds, so I don’t deserve help getting out of it. But that’s not healthy at all, so I’m going to try to resist it. I’d like to do some research on ketamine troches tonight so that I know more about what to expect, and then I’ll try to pick them up from the compounding pharmacy tomorrow. Ketamine seemed to stop working for me after a while, so I’m interested to see whether taking a break has impacted its efficacy.
Writing has always been helpful for me, but I’m finding the motivation to do it hard to come by. When I was more actively questioning my diagnosis, having a written record of my symptoms and how different treatments have affected me was incredibly useful in trying to piece together a timeline, so I’m going to renew my efforts to keep up with my blog. It might come in handy later.