In light of my recent posts, I thought it might be useful to elaborate on the levels of mental health care you can find in a hospital setting (at least in the US). What are the differences between them, and what can you expect from each?
Inpatient Treatment
Entering a hospital as an inpatient for mental health care can be incredibly nerve-wracking. If you don’t know what to expect, the experience is overwhelming. The important thing to remember is that the system is designed to keep you and the other patients safe.
In an inpatient setting, you sleep at the hospital and spend your days on the unit. You might have a roommate; they’re probably just as overwhelmed as you are. The staff will likely elaborate on the expectations for patients, but you may be expected to spend the majority of your time in a common area, interacting with other patients and staff. Your nurses and doctors will want to see that you’re participating in group therapy, willingly spending time outside of your room, and eating meals with the unit. You’ll meet with your doctor and a social worker, and have a chance to discuss your treatment goals and any concerns you have. Different hospitals have different timeframes for this; you could meet with your doctor as often as every day, although it may happen less frequently.
Before you’re discharged, the staff will probably want to be sure that you have a support system, safety plan, and aftercare set up. Continuing mental health care might look like a partial hospitalization program, intensive outpatient program, or outpatient therapy with your own mental health counselor.
Partial Hospitalization Program (PHP)
The next level down from inpatient care is a partial hospitalization program. In a PHP, patients typically attend therapy for most of the day, sleep at home, then return for the next day of programming. For example, the PHP I did was from 9 am to 3 pm, Monday through Friday for ten days.
Programming usually focuses on teaching skills and information you can use to manage your illness. The PHP I was in took content mainly from DBT, although we also touched on ACT and CBT. You’ll meet with a psychiatrist and your case manager, who is usually one of the therapists who leads group discussions and teaches content. Your case manager will probably set up a treatment plan with you, and meet with you periodically to check in on your progress.
Many people come to a PHP through inpatient hospitalization. After spending time isolated from your normal, day-to-day life, it can be overwhelming to be tossed back into it. A PHP can serve as a helpful step-down to ease you back into your routine. Other people come straight from their outpatient treatment. They may not need the level of mental health care you get with inpatient treatment, but the support of a PHP can give them the structure they need to stay safe.
Intensive Outpatient Program (IOP)
In the same way that a PHP offers a transition from inpatient back into your normal life, an IOP does the same. It’s the next level down from a PHP, but is still, well, intensive. An IOP is similar to a PHP in the content that’s taught, but you meet less frequently and for a shorter amount of time each session, but for a longer overall duration. Many IOPs meet three times per week for three hours. The program might run for as many as eight weeks. The IOP at the hospital where I did my partial hospitalization had a more independent treatment; you didn’t get to meet with a psychiatrist or a case manager. That meant you would need to have outside medication management set up for your time in the IOP.
Many people go straight from inpatient treatment to an IOP, although others may need the structure of a PHP. Some people continue on from partial hospitalization to intensive outpatient, but sometimes that’s not feasible with work or family obligations. I decided not to do an IOP, but rather to return to my regular schedule and leave IOP as an option should I need more intensive mental health care down the road. It’s all very individual, and which program you choose depends on your specific needs and constraints.


 There is always a choice. Two therapists have told me this independently. It took a little while for the meaning to sink in after the first therapist said it. I had gone a few weeks without self-harm at that point, and I still felt utterly controlled by it. The question of whether to do it or not didn’t seem like a choice; it seemed like an inevitability. Over time, the less trapped by it I felt, and the more sense that statement made. Although the choice of whether to self-harm might have been stacked in favor of doing it, the choice to take steps to change that was still mine.
There is always a choice. Two therapists have told me this independently. It took a little while for the meaning to sink in after the first therapist said it. I had gone a few weeks without self-harm at that point, and I still felt utterly controlled by it. The question of whether to do it or not didn’t seem like a choice; it seemed like an inevitability. Over time, the less trapped by it I felt, and the more sense that statement made. Although the choice of whether to self-harm might have been stacked in favor of doing it, the choice to take steps to change that was still mine.
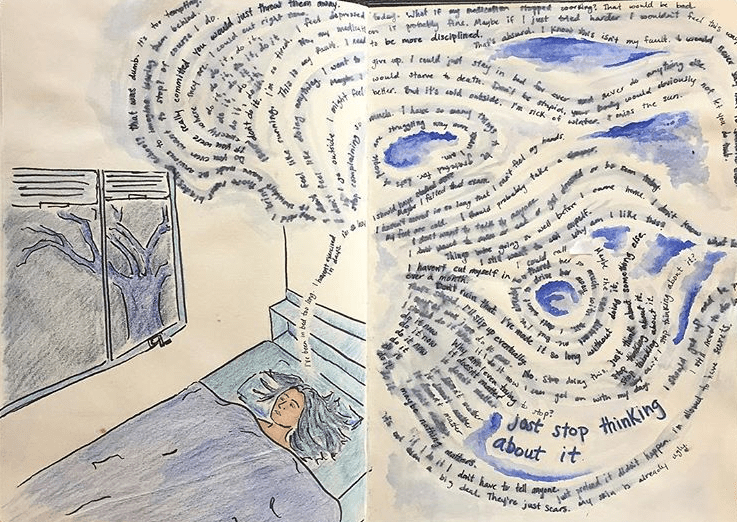

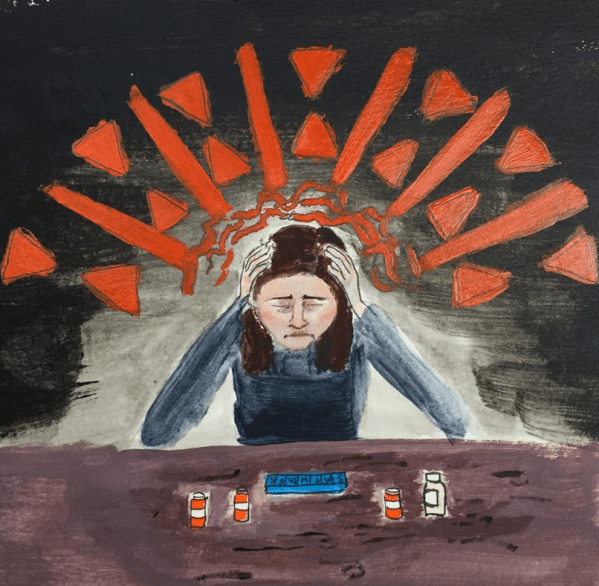 It’s nothing to be ashamed of I tell myself twice daily. What day is it? They all blend together. I open the third compartment, pour the pills into my palm, wait for a moment. Maybe this day will be the day. Maybe if I give the medicine a moment of silence; infuse it with my desperation before I let it fall down the dark well of my esophagus.
It’s nothing to be ashamed of I tell myself twice daily. What day is it? They all blend together. I open the third compartment, pour the pills into my palm, wait for a moment. Maybe this day will be the day. Maybe if I give the medicine a moment of silence; infuse it with my desperation before I let it fall down the dark well of my esophagus.